
Content Sections
By Rob Verkerk PhD
Founder, executive and scientific director, ANH-Intl
Scientific director, ANH-USA
Co-chair, Health & Humanity Committee, World Council for Health
Topline
- WHO case definitions are set up perfectly to mask immune suppression that reflects covid-19 jab injury such as the increasing prevalence of shingles following covid-19 injection
- Imagery being used by global media are not representative of current international cases of monkeypox and have been recorded incorrectly by CDC and Getty Images that are the sources
- Next-generation smallpox vaccines are almost ready for global roll-out and are likely to be justified as necessary by health authorities despite a lack of evidence of safety, let alone interactions with ‘genetic vaccines’
- International agencies have already engaged in a monkeypox simulation that draws heavily on the covid playbook and Bill Gates’ newly released book, How to Prevent the Next Pandemic
- Whether monkeypox gathers momentum or dwindles, its timing is ideal to justify further support for global, centralised health governance orchestrated by the WHO through the International Health Regulations and the WHO ‘pandemic treaty’
The current World Health Organization (WHO) suspected case definition of monkeypox is broad enough to include anyone with covid or a common cold, who also have a shingles rash. As it happens, there are a large number of people out there who have suffered immune suppression from covid-19 injections, who also sport a shingles rash.
Should we be worried? We think so, but not about monkeypox itself. Much more about what the WHO and collaborating institutions, governments and corporations are up to. A lot of ‘truth seekers’ will have already found out about the WHO tabletop exercise in 2021and it is without doubt interesting that the 15 May 2022 date is given as the 'attack' date of the monkeypox outbreak. But let’s look beyond that.
Let me explain.
What’s in the news...
Yesterday, BBC News reported the following on the monkeypox outbreak: “More than 100 cases of the virus - which causes a rash and a fever - have been confirmed in Europe, the Americas and Australia….The virus has now been detected in 16 countries outside Africa….. a top EU health official has warned that some groups of people may be more at risk than others…..Dr Ammon suggested that countries should review the availability of the smallpox vaccine which is also effective against monkeypox.”
Has the BBC reverted to its past reputation as a balanced reporter of news? That would seem unlikely in the present circumstances.
Especially when the BBC is partially funded by the Gates Foundation and it opts to use a Getty Images photo of an unconfirmed monkeypox case that may actually be smallpox (which you'll get to see as you read on, in Fig. 5 below).
How far back does WHO and BBC misinformation, disinformation or malinformation go?
Yesterday’s BBC News piece contained a powerful image of the arm and leg of a pox-covered child (Fig. 1).
Driven by concerns that this looks very much like smallpox (check out the UK Health Security Agency images [shown also in Fig 5B] which is closely associated with the Hospital for Tropical Diseases and you’ll get a more representative view of the clinical features of human monkeypox ), I was keen to dig deeper.
The Getty Images caption tells us:
“BONDUA, LIBERIA - UNDATED: In this 1971 Center For Disease Control handout photo, monkeypox-like lesions are shown on the arm and leg of a female child in Bondua, Liberia. The Centers for Disease Control and Prevention said June 7 the viral disease monkeypox, thought to be spread by prairie dogs, has been detected in the Americas for the first time with about 20 cases reported in Wisconsin, Illinois, and Indiana. (Photo Courtesy of the CDC/Getty Images)”
We’ve been unable to find a place called Bondua in Liberia. There is however a Bondua in Sierra Leone. Is that what the CDC means? Isn’t it a bit like saying the case was reported from London in France - leaving everyone confused about place and country? Not quite, actually, as there is a London in France, just no Bondua in Liberia.
You might think I'm splitting hairs. But such details are actually critically important when they're being communicated to a worldwide audience that's waiting with bated breath to understand the implications of yet another infectious disease outbreak.
Sierra Leone did in fact boast the highest incidence of smallpox in the world between 1967 and 1968 and we've unearthed some genuine red flags as to the origin of this CDC/Getty Images photo. By 1971, it appears smallpox had disappeared from Sierra Leone. And, as an add-on, contrary to what the vaccine PR machine likes to suggest, the historical record does not provide evidence that it was mass vaccination as part of the WHO’s Smallpox Eradication Program that caused infections to decline then disappear from Sierra Leone. More on that later.

Figure 1. Photo used by BBC News (and many other mainstream media) showing pustular lesions of monkeypox or smallpox in a young girl, suspected to be 4 or 6 years old in 1970 or 1971 (based on case reports – see Fig. 2). Photo reportedly from Bondua (Sierra Leone) or the Grand Gedeh rainforest region of Liberia. Courtesy: CDC Public Health Image Library.
So we dug deeper again.
Bingo – we found the case reports of the 20 known monkeypox cases between 1970 and 1975 – published in none other than the peer reviewed Bulletin of the World Health Organization back in 1976.
We were surprised to find no reported case of a young girl from either Sierra Leone or Liberia in 1971, the date given by the CDC. There were however two cases reported in Liberia the year before (Fig. 2).
If the pustulated girl was aged 6, the case wasn’t confirmed. If she was 4, the case was confirmed by electron microscopy and it was isolated (Fig 2). But this 4-year-old girl was also positive for smallpox. So did the CDC get the country wrong – and the date? Or are we looking at a smallpox case somewhere in West Africa in 1971? Or 1970? Or from elsewhere? Who knows?
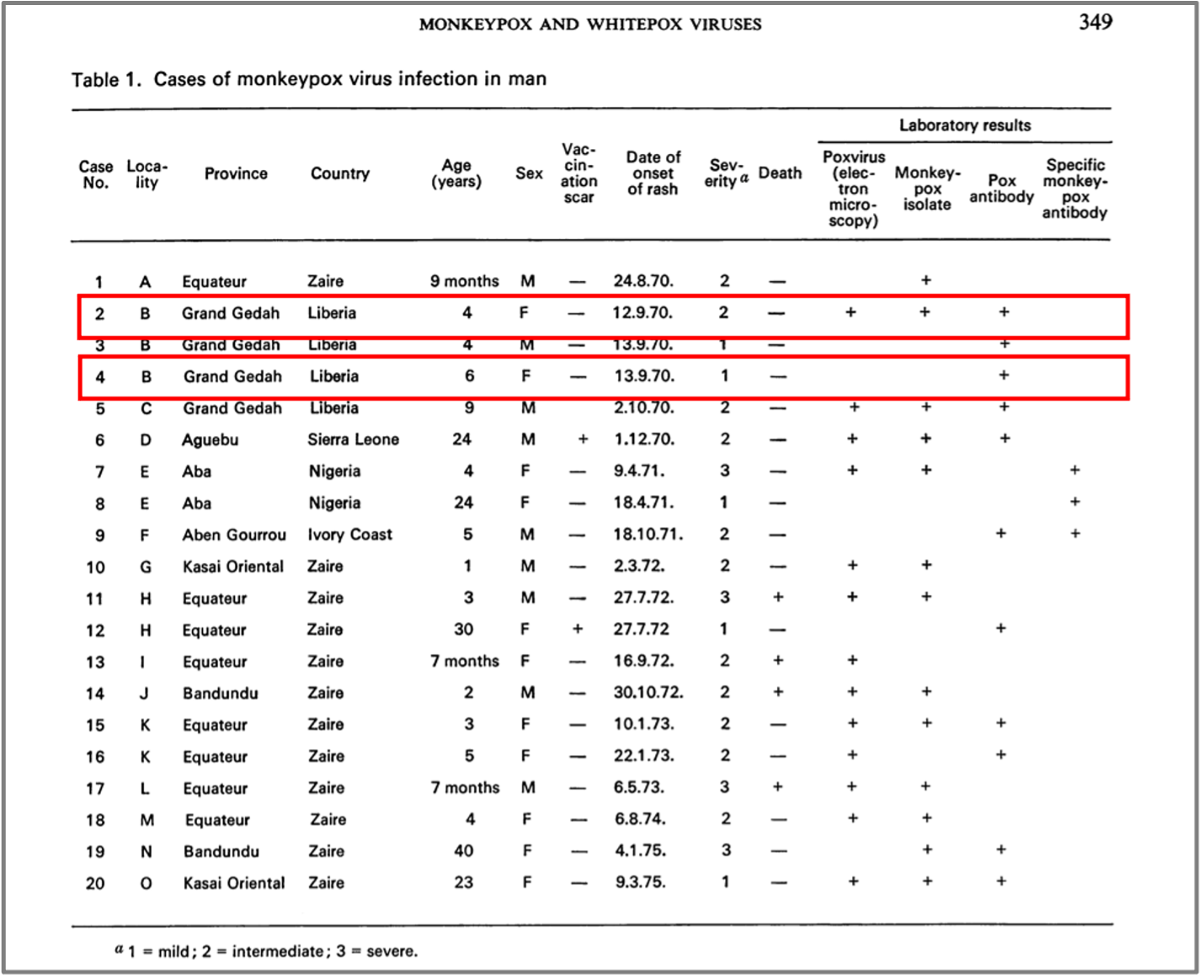
Figure 2. Reported suspected or confirmed monkeypox cases. The two known cases of young girls are highlighted in the red boxes. Both are from the Grand Gedeh county of Liberia. Source: Arita & Henderson (1976). Note that monkeypox was not confirmed by electron microscopy, isolation, or serology (antibodies) in the 6-year-old’s case, and both were positive for smallpox antibodies. There is also a misspelling in the paper of Grand Gedeh.
In the world of scientific rigour I grew up in, one in which I’ve been immersed the entirety of my working life, I would reject the CDC image as a reliable illustration of monkeypox given the inability to prove its authenticity. That’s before we even look more closely at the clinical features (see Fact 7 below). It should be declared ‘scientific misinformation’, especially when used by the BBC and other mass media to whip up fear of monkeypox.
It’s funny how quickly the tables can turn. I can see the meme already – and what a pleasant surprise, our media team has just knocked up exactly what I saw in my mind’s eye….

With amendments to the International Health Regulations (IHR) floating in the balance, and these regulations along with the WHO ‘Pandemic Treaty’, also up for discussion, we (the people) need to be hyper-vigilant. The IHR and the proposed treaty will give the WHO unprecedented executive powers to declare an international health emergency at its own discretion, then organise and deliver a response that overrules any that a sovereign nation might consider fit. It might sound a little old school, but that’s what we used to call an authoritarian regime, and authoritarianism and optimal health care aren’t good bedfellows because there just isn’t enough flex to deal with local circumstances, capacity and resources.
At ANH, we don’t deal in fear porn. Nor do we feel the need to exaggerate scientific or factual information. But that doesn’t stop us speculating as to what the new global health authoritarians might be planning for us.
Now that we’ve determined we can’t trust the CDC, Getty, the BBC or the WHO, let’s look at some clear facts, then speculate.
Facts
Fact 1 – case definition of suspected case
The current, case definition (last updated on 22 May 2022) of a suspected case of monkeypox given in the WHO’s interim guidance implies the following:
Suspected monkeypox case = unexplained rash AND (headache OR fever OR swollen lymph nodes OR muscle/body aches OR backpain OR profound weakness) AND any kind of raised (papular) or blistered (vesicular) rash.
Fact 2 – case confirmation via a PCR test
Yes, you’ve guessed, a Real-Time PCR test. Genomic sequencing and surveillance - which has serious limitations as a method for diagnosing disease - will trump any presentation of clinical features. Straight out of the covid-19 playbook.
Fact 3 – other conditions that might meet the case definition of a suspected case
That’s easy. How about:
- Covid-19, flu, common cold or any number of other commonly circulating respiratory or other infections, coupled with shingles (which is caused by the varicella zoster virus).
- Or a person with flu who trips up and falls in a nettle (Urtica dioica) bed.
- Or a person whose immune system is suppressed following repeated exposures to covid-19 injections and develops shingles.

Figure 3. An example of a shingles rash developed following Covid-19 mRNA injection. Source: Eid et al. J Med Virol, 2021: 3: 10.1002/jmv.27036.
Shingles is being widely reported among those who’ve had covid-19 injections. See reports here and here. And of course you’ll then find the systematic review and meta-analysis that denies any such relationship!
Do you still trust in science? As odd as it sounds, I still do. It’s just that scientism and the corporatocracy are doing their darndest to corrupt what is a useful methodology for understanding many aspects of the world around us.
Fact 4 – monkeypox cases have been increasing steadily in West and Central Africa since 2007
The news that privileged people in Western industrialised countries (mainly men who have sex with other men [MSM]) have now become infected outside of West and Central Africa may be newsworthy. But monkeypox infection has been rising steadily in Central Africa (here and here), the largest number and increase of cases being in the Democratic Republic of Congo.
What about the next fact, then?
Fact 5 – monkeypox cases appear to have disappeared in West and Central Africa
The latest ‘heatmap’ of monkeypox cases from Global.Health is shown in Figure 4. Global.Health is a data science initiative created in partnership with institutions like Johns Hopkins, Harvard, Oxford Uni, the Rockefeller Foundation and others heavily involved with the analytics and response to covid-19 globally.
Is it a case of: if you don’t look for it, you don’t see it?
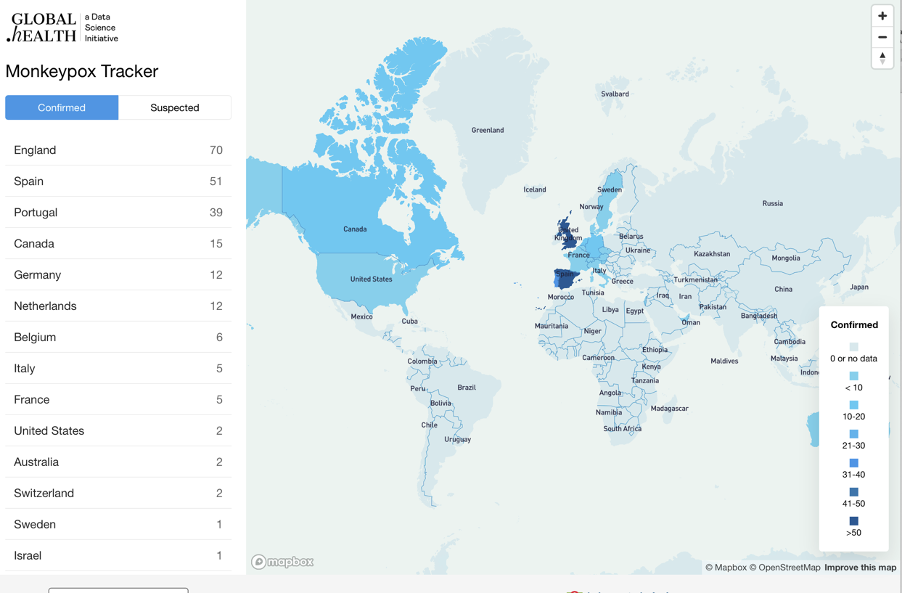
Figure 4. Global.Health heatmap for human monkeypox as of 25 May 2022. Source: Global.Health
Fact 6 – there are two genetic variants of monkeypox that pose different risks
The variant (clade) of monkeypox that’s circulating internationally at present, the West African clade, is the less deadly of the two known clades of the monkeypox virus (MXV). The other is the Central African clade. The West African clade is reported to have a case fatality rate of around 3.6%, as against 10.6% for the Central African clade.
There has also been a change in age of those who appear primarily susceptible, with infections in the 1970s being reported mainly in young children. Now, increasingly, young adults may also be affected.
Could there be significant genetic drift in the West African clade that now makes it more transmissible, and more likely to affect older age groups who engage promiscuously? Could a lab have been involved at some stage? Has there been genetic transfer from an animal reservoir? It's too early to know, but various labs have been engaged in MXV research and animal (especially monkey) reservoirs are well known.
Fact 7 – WHO’s original descriptions of smallpox and monkeypox pustules suggest visual differences
Check out page 18 of WHO’s ‘Restricted Circulation’ document from 1973 that is now in the WHO archives in its full manually-typewritten, Helvetican glory.
While the description suggests Vaccinia (smallpox) pocks at 72 hours are “3 to 4 mm in diameter, flattened with central necrosis and ulceration, and sometimes slightly hemorrhagic”, the description of human monkeypox pocks are “about the same size as those of variola, but they are not as raised; and most of the pocks have a pinpoint hole in the center and are sometimes hemorrhagic.” [bold is our emphasis]
Then there's the comparison between what the CDC, BBC and others are showing us about the clinical features, versus a more representative view, as given by the UK Health Security Agency (Fig. 5).

Figure 5. Comparing A. CDC monkeypox image used by BBC and other global media channels that appears more like a typical presentation of smallpox (Source: CDC), with B. the more representative images provided by the UK Health Security Agency (Source: UKHSA).
Fact 8 – the world is gearing up for roll-out of an updated smallpox vaccine
‘No shit, Sherlock’, excuse my English. This WHO report of an experts’ meeting in November 2021 (published in January 2022) contains some interesting insights. It includes discussion around the new Bavarian Nordic MVA-BN attenuated vaccine and a fourth generation recombinant (genetically modified) DNA vaccine, born and bred in Russia, VACΔ6.
The Russia/Ukraine war may not work in favour of VACΔ6 roll-out in the Western world.
Then there’s ACAM2000® manufactured by Sanofi Pasteur Biologics that’s already licensed in the USA, Australia and Singapore. According to the WHO, “Serious adverse effects [have been] reported from clinical trials with ACAM2000 include myopericarditis and cardiomyopathy.”
The US and the UK are stockpiling smallpox vaccines.
Profiteers in both the vaccine and antiviral sectors are widening their pockets in preparation for receipt of fear-induced revenues. The covid-19 corporatocracy playbook is now well and truly oiled. One such player, Emergent Biosolutions, was set to make a killing (excuse the pun) on covid-19 vaccines but lost out when an FDA inspection found its manufacturing plant was contaminated. It’s now getting ready for a second attempt at glory.
Even though the world will likely be told that smallpox vaccination is ‘safe’ (note the CDC’s spin on live virus vaccines), the history of previous smallpox vaccines suggests a different story, this 2003 review reminding us there are “several known side effects that range from mild and self-limited to severe and life-threatening.”
The ‘new boys on the block’ are not shy of talking about the need to find use deficiencies of previous vaccines, from serious side effects through to inducing replication of smallpox virus in the bodies of the vaccinated.
The authors responsible for the recombinant VACΔ6 at the State Research Center of Virology and Biotechnology in Russia stated in a paper published in 2017 that smallpox virus is “considered a potential agent of bioterrorist attacks, which could have catastrophic consequences for the entire world population. The lack of effective antiviral drugs and the risk associated with conventional VACV-based live vaccines, because of severe postvaccinal complications, necessitate the development of modern, safe orthopoxvirus vaccines and protocols for their use.”
Fact 9 – the monkeypox game was released last year
You likely already know about this – thank you ‘new media’. But it was just over a year ago that the Nuclear Threat Initiative (NTI) carried out a tabletop simulation exercise in partnership with the Munich Security Conference on a new variant of monkeypox. The NTI is described by Wikipedia as “a nonpartisan, nonprofit organization founded in 2001 by former U.S. Senator Sam Nunn and philanthropist Ted Turner in the United States, which works to prevent catastrophic attacks and accidents with weapons of mass destruction and disruption – especially nuclear, biological, radiological, chemical, and cybersecurity.”
The simulation exercise drew heavily on the covid-19 playbook, but has added elements from Bill Gates’ new book, ‘How to Stop the Next Pandemic’. The probability that this is a coincidence is likely low.
Fact 10 – smallpox decline and smallpox vaccination
In Figure 6, I’ve taken official WHO data reported by Our World in Data and inserted the dates in which the WHO’s global Smallpox Eradication Program was started and completed.
As the text on Our World in Data explains, “Europe, North America and Australia managed to eliminate smallpox relatively early, most by the 1940s (predating the WHO’s Intensified Smallpox Eradication Program, which was launched in 1966).”
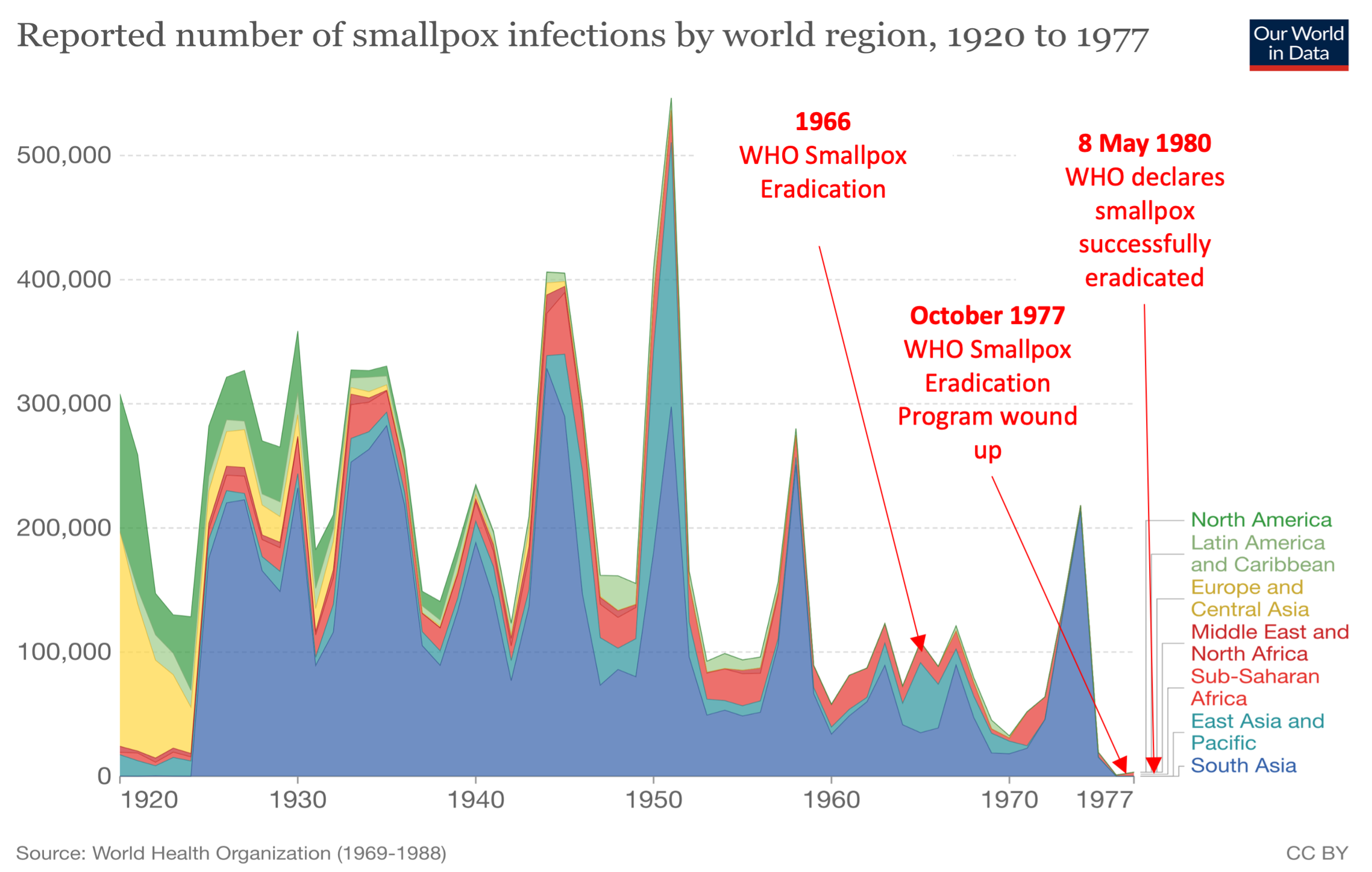
Figure 6. The decline of smallpox globally and dates of inception and closure of WHO Smallpox Eradication Program. (Sources: Our World in Data and Nature, Nurture and Chance: The Lives of Frank and Charles Fenner
Speculation
With these 10 pieces of factual information, what are we to make of it all?
We can only guess. I see three main areas worth speculation.
Speculation 1 – origins
Monkeypox virus (MPXV), a zoonotic, double-stranded DNA virus belonging to the Poxviridae family was first discovered in monkeys shipped from a lab in Singapore to one in Denmark in 1958. Following its first discovery in humans in 1970 in the Democratic Republic of Congo, it was regarded as being “endemic to the heavily forested regions of West and Central Africa”.
It is interesting that confirmed cases are now all outside of Africa. Git.Hub, at close of play today (25 May 2022), indicates 228 confirmed cases and 89 suspected cases; none in Africa.
It's now circulating outside the forested regions of Africa, and it’s getting a little bit of a foothold in some Western countries, especially among gay and bisexual men. The rashes are reported as generally mild, and it's no surprise that initial sequences of the genome of the new cases suggest they originate from the West African clade. But by how much does it differ? And is it conceivable that monkeypox has been tampered with in a laboratory? Short answer: Yes. Longer answer: too early to know one way or another.
Speculation 2 – planned scenario: push smallpox vaccination with a backdrop of fear over monkeypox
Given the public is now regarded as a good substrate for fear porn, it is clear the machine of global health is moving towards rolling out smallpox vaccines arguing they confer some cross-immunity to monkeypox. This is despite clear evidence that monkeypox failed to develop into significant outbreaks in the absence of smallpox vaccination. Fine and colleagues, writing in the International Journal of Epidemiology in 1988 said, “current evidence indicates that the virus is appreciably less transmissible than was smallpox, and that it will not persist in human communities, even in the total absence of vaccination. The findings thus support the recommendation of the Global Commission for the Certification of Smallpox Eradication to cease routine smallpox vaccination in monkeypox endemic areas, but to encourage continued epidemiological surveillance.”
We should start to expect a large push on smallpox vaccines given they are already available. This will require any survival conscious human to re-engage with the history of smallpox vaccination that has faced years of controversy and whitewashing.
You could argue, as many do, that the decline in smallpox in Europe, North America and Australia was linked to national roll-outs of Edward Jenner’s vaccine in Europe and North America. If so you’d call yourself a believer in old school, live vaccines, but your belief would not serve you well if you tried to superimpose it on modern day smallpox vaccines.
If you were of this persuasion, you might also like to delve into Alfred Wallace’s report ‘Vaccination Proved Useless & Dangerous – from Forty-five Years of Registration Statistics’ published in 1889. It might question your belief or suppositions. The 133-year-old report also serves as a reminder that we haven’t come as far in our understanding, or our ability to determine causation, as many would like to think. Others may already be familiar with Dr Suzanne Humphries and Roman Bystrianyk’s important, information-laden and controversial book ‘Dissolving Illusions’ which devotes its fourth chapter to Smallpox and the First Vaccine. If you still believe in balance, don’t be frightened of reading something that counters everything you might have previously heard.
Smallpox was deemed eradicated in 1980 despite considerable evidence that mass vaccination in Western countries was largely irrelevant and induced some dire adverse reactions. While the ‘ring vaccination’ principle is often hailed as a major factor in driving out remnant infections in developing countries, given that smallpox disappeared in the absence of vaccines through much of the developed world, it’s not a strong argument scientifically.
You can make up your own mind as to whether any available data show causality, association or none of the above. But it beggars belief, at least my belief, that schoolchildren in Europe, North America and Australia are still taught through their formal curricula that smallpox vaccination – as the only known potentially fatal infectious disease to have disappeared - was the world’s most effective vaccination program. This viewpoint was used to coerce young people to receive covid-19 injections yet is entirely irrelevant given the inability of covid-19 ‘vaccines’ to induce herd immunity.
All of this suggests that health-aware people need to be very wary of the likely governmental and social push for new smallpox vaccines in the wake of monkeypox hype. Available data suggests we should not buy into the notion that historical smallpox vaccination was safe or even effective despite this view being perceived as a truism through its repetition over decades. Depending on your circles, you may also have heard of another oft-repeated notion, that ‘vaccination causes autism’. Whether we’re talking autism or smallpox, rather than dismissing or blindly accepting either as truisms, we owe it to future generations to apply science to such crucial issues. Not turn them either into mantras or taboos. Cancel culture and censorship unfortunately do nothing to assist such scientific discourse but at least ‘new science’ is reorganising itself, as we saw at last weekend’s Better Way conference.
Speculation 3 – global health powergrab
For many of us, this is where it’s all leading. The Epoch Times makes a good argument in this vein.
Monkeypox could peter out in the industrialised world of its own accord (no doubt alongside claims that the WHO global response won the day). Or it might gain even more of a foothold. Either way, it could serve as a perfectly timed reminder to people for why global responses involving pharmaceutical weapons are so important. Despite no evidence that they were required, or were definitive, in the decline of covid-19, smallpox, or numerous other infectious diseases.
If you were standing in Tedros’ or Gates’ shoes, you’d no doubt be thinking the timing and nature of the monkeypox outbreak was spectacular. Too spectacular, perhaps, to be coincidental? But then again, they’ll know many things we don’t.
But yes, as I scribe this, the World Health Assembly is engaged in its 75th meeting and is attempting to get agreement on amendments to the International Health Regulations (IHR). This feeds directly into efforts to get sovereign nations to support the drafting of the WHO ‘pandemic treaty’ which aims to be adopted in 2024. The last opportunity for public comments on the draft appears to be the 16th and 17th June 2022.
For a great account of what’s going on, there are few better sources than Dr Silvia Behrendt, former consultant to the International Health Regulations Secretariat at the WHO, currently director of the Global Health Responsibility Agency (CHRA) and one who is alive to the planned shift to centralised and authoritarian control of human health – from Geneva.
Following are two key links from the GHRA:
>>> About the International Health Regulations
>>> From surveillance to ‘Public health emergency of international concern'
Then there’s a great article by Dr Silvia Behrendt and Dr Amrei Müller about the WHO ‘pandemic treaty’. And another by the same authors on what is going on at the time of writing at the 75th World Health Assembly regarding the IHR.
Speculation 4: our response
I’m not a big one for laying out guerrilla strategy in the public domain, given how we’re all being observed in this ultra-surveilled world.
I’d just say this: they want people they call ‘anti-vaxxers’ (the majority of which could equally be called ‘health conscious individuals with free thinking minds’) to respond in particular ways. That includes focusing endless amounts of energy trying to stop processes like pandemic treaties that are entirely undemocratic. I’m not saying it’s not worth trying, but we’d be lucky in my view to find clear success if this was our only strategy.
We should also remind people that the ideology that underpins the use of fear and manipulated science to engender support for the global control of health is deeply flawed.
But we must do so much more as well. That includes building parallel systems of health and care, new bioethical frameworks, new educational systems, new food systems, new media – and a host of other things. Things that are for us, not for them.
You know the adage, whatever you focus on becomes your reality. Tony Robbins makes the same point: where focus goes, energy flows.
We must do everything we can to avoid engaging with this attempted transition to global health governance, while building parallel structures that work with, not against, health, food and the people.
So let’s focus on all the other things we need to do as well – all of them central to ANH’s mission.
Thank you for reading this far! In gratitude to the growing number of people who are awake.
Please share this article as widely as you can. You can re-post or publish, as long as you make a clear indication of the source, as clarified in our republication statement below.
>>> Alliance for Natural Health International re-Publishing Guidelines
>>> Has this article generated questions for you? Did you know our ANH Pathfinder Members get a free monthly Q&A as part of their annual membership? Why not Join us!
>>> Visit covidzone.org for our full coverage of the coronavirus crisis and beyond
Proudly affiliated with: Enough Movement Founding coalition partner of: World Council for Health




Comments
your voice counts
26 May 2022 at 9:02 am
brilliant and helpful as ever. Thanks Rob!
26 May 2022 at 9:16 am
Here we go again, this should be re-named moneypox!
26 May 2022 at 12:29 pm
Funny you should say that Pauline. One of the first things Dr Ryan Cole shared about it at the #BetterWay Conference is the that K in monkeypox is silent... ;)
We shall always prevail!
Meleni
26 May 2022 at 1:46 pm
Superb piece, putting all the pieces together so succinctly. Thank you.
26 May 2022 at 6:34 pm
Thank you once again to all at ANH for your tireless and diligent work.
So much gratitude.
26 May 2022 at 9:53 pm
Dr. Rob,
Great article!! Keep up the good work,
David Brownstein, M.D.
26 May 2022 at 10:54 pm
A very well assembled piece Rob. Thanks for the clarity!
26 May 2022 at 11:02 pm
Thank you for your article.
Here's something rather heavy for the average person, but for someone with scientific training, it's right on
https://besovereign.com/greenmedinfo/greenmedinfo?recording_id=908
27 May 2022 at 12:09 pm
Perfectly pitched balance of facts, analysis, quiet cynicism , tongue firmly in cheek sarcasm, realism, practical guidance, and most touchingly, positive hope.
Now you are really motoring Dr R. Thank you.
29 May 2022 at 4:01 pm
Thanks Rob! Excellent article - who would have guessed that Smallpox vaccines are almost ready to be rolled out?! 🤣
31 May 2022 at 10:30 pm
So grateful to have someone voice and put in to order my thoughts and do all the hard work researching the facts. For me reading your words helps me to feel I am not alone in this situation trying to protect my health.. I am also taking energy that from todays evil we are growing and creating a better world. We will prevail. Thank you for your courage ANH.
04 June 2022 at 1:19 am
You have done a wonderful job at putting all the research points and commentary into perspective for the well educated, but the majority of today's society will not be able to understand what u have written, unfortunately. This inability to understand is only due to the 'dumbing down' of our younger generations within our public schools. The people that understand what's written here without any clarification of the vocabulary used are the minority of the people that will voluntarily pick up arms (if needed) to defend everyone's right to decide upon their own healthcare. Please make this more understandable to the lay person and you may have the backing of a majority of the people you need to make a stand on this.
05 June 2022 at 1:40 pm
Is it suspicious that a tractor trailer load of lab monkeys crashed on Rt 80 back in January, 2022 near Danville PA? A woman stopped to see if she could help and was told by the driver that the cages were filled with cats. Being a cat lover, the woman went to check out the cages strewn about the highway. To her surprise a monkey hissed at her from close range. She had been walking through feces and apparently came down with cold symptoms soon after. Three monkeys escaped, but I believe they were found.
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences