

Content Sections
By Rob Verkerk PhD, ANH-Intl founder, scientific & executive director
Topline
- Lockstep political decision to role out leaky ‘vaccines’ occurred around the world immediately following omicron announcement
- Circumstances with a new, heavily mutated variant, vastly different population immunity and knowledge about ‘genetic vaccine’ effectiveness, nothing like those 12 months ago when first generation covid injections were rolled out globally
- Omicron may be more infective, is likely no more dangerous, but may be more likely to evade injection-induced immunity
- There is no conclusive evidence that omicron originated in Africa – which happens to have the lowest injection rate and case rate of covid-19
- Mass injection of first gen injections, followed by re-worked omicron-specific jabs, could cause disastrous consequences, including accelerating development of further variants and antibody-dependent enhancement (ADE) of disease
- We consider some of the possible political and economic drivers behind the new unscientifically backed policy to up the ante on injections.
No sooner had the Omicron hysteria hit the headlines, politicians, aided by a compliant global lockstep media, started telling the world’s population to prepare to roll up their sleeves. What’s more, three scapegoats have been identified: the unvaccinated, HIV patients and the least vaccinated continent on the planet: Africa. One of many similar calls was made in the influential Scientific American magazine by Southampton University public health and vaccine hesitancy researcher, Michael Head PhD, not unsurprisingly a Gates Foundation funding recipient.
For many in the industrialised world, there is a sense of déjà vu from this time last year – but with a twist. Last year the population had been primed to expect almost impossibly high levels of protection from infection based on the results of phase 3 clinical trials. Only recently have these trials been brought into question. Last year, the majority had also bought the line that these new generation ‘genetic vaccines’ would stop transmission and yield herd immunity. The head of the Oxford Vaccine Group, Professor Andrew Pollard, subsequently recently told the world that possibility is now “mythical”. Knowing what they knew then, people flocked to the vaccination centres as the promise being offered was a return to normal life. Only time would tell how misplaced that view was.
This time around things are very different. The covid-19 injections have been shown to increasingly fail even with delta, hence the re-casting of the ‘vaccine effectiveness’ correlates from protection against infection now to protection against severe disease. The indisputable reality is that the covid-19 injections are ‘leaky’. The spike-targeting neutralising IgG antibodies they so readily elicit just don’t neutralise (block) very well so they can’t stop infection or subsequent transmission.
What drives the creation of immune escape variants?
Perceptions among politicians, the public and even scientists as to the main drivers of mutations that can escape the effects of the immune system, whether from naturally-acquired infection or the response generated by injections, differ wildly. Smack in the middle of this lack of consensus comes Omicron, and a high chance that policies based on one line of thinking will be viewed as counterproductive or even potentially disastrous and life threatening by others.
We’ve reported on the underlying science at length before, and supported the evolutionary arguments elaborated in the public domain by Belgian vaccinologist, Geert Vanden Bossche VDM PhD. David Lorimer, Programme Director of the Scientific and Medical Network, and I have this week released a short article that attempts to summarise in layperson’s language the central tenets of Dr Vanden Bossche’s thesis.
The opposing arguments ignore entirely evolutionary pressure and focus on the unvaccinated and the immune compromised as the reservoirs that provide more opportunities to breed mutants. The logic – at face value – seems reasonable. If the virus is able to replicate more often in people who suffer covid-19 disease for longer, and people who can’t effectively neutralise the virus, the increased replication increases the probability of mutants emerging. More rolls of the dice, if you like. The trouble is that this argument is fundamentally flawed for a number of reasons.
“The immediate decision to foist the old injections on the public to ‘boost’ immunity with what are probably even more weakly neutralising antibodies at best is clearly based on political or economic, not medical, expedience.”- Rob Verkerk PhD

We’ve seen previous mutants by and large being generated under high vaccination pressures, with increases in cases being associated with expanding ‘vaccine’ coverage. Also, clear evidence that the vaccines are increasingly unable to neutralise the virus, especially more recently emerging variants, so being unable to stop transmission while also waning in effectiveness within a few months post-jab. What’s more, they also interfere with innate immune training which is our primary defence against different variants of this (and other) pathogens and our only means of developing herd immunity given the 'leakiness' of the current 'genetic vaccines'.
Omicron focus
In a sea of immense uncertainty, one thing that is more or less certain, now that the initial errors in the claimed mutations were corrected, is the 32 spike protein mutations of Omicron. But it’s not just the, comparatively speaking, high number of significant mutations in the spike protein (Table 1), it’s their potential impacts on both the virus and the human immune systems with which the virus interacts that are key. It’s of course too early to know exactly what effects these mutations will have on the very diverse and varied populations of humans, and potentially other species if spill-over continues.
Table 1. SARS-CoV-2 ‘variants of concern’
|
Variant |
Spike protein mutations |
Earliest documented samples |
No. of countries reporting |
|
Omicron (B.1.1.529) |
32 |
Multiple countries* (11/21) |
20† |
|
Delta (B.1.617.2) |
10 |
India (10/20) |
196 |
|
Gamma (P.1) |
12 |
Brazil (11/20) |
103 |
|
Beta (B.1.351) |
10 |
South Africa (05/20) |
146 |
|
Alpha (B.1.1.7) |
11 |
UK (09/20) |
197 |
Main data sources: WHO and GISAID.
* Note that the WHO has not claimed either Botswana or South Africa as countries of first documentation; see discussion below.
† Based on media reports by Dr Anthony Fauci
The limited information available from the small numbers of cases that have been reported so far is that disease severity (i.e. deadliness) is not significantly greater than with delta. It’s too early to say if omicron will out-compete delta as this depends on many factors, such as the ability or otherwise of omicron to evade innate and/or adaptive immunity in populations with different immune backgrounds (generated by covid injections and naturally-acquired infection), and latency prior to high viral loads being generated.
Early reports, such as those by the South African doctor, Dr Angelique Coetzee, who first spotted the new symptoms of omicron-mediated covid-19 were that the severity of disease wasn't worse than delta. It's likely though that the pattern of symptoms will be different. Younger people may also be more vulnerable, especially if their trained innate immunity is damaged by injections. This view is of course not wholly in line with that of the WHO that stated the following:
"There is currently no information to suggest that symptoms associated with Omicron are different from those from other variants. Initial reported infections were among university students—younger individuals who tend to have more mild disease—but understanding the level of severity of the Omicron variant will take days to several weeks”.
‑ World Health Organization, 28 November 2021
Many independent experts have opined that transmission might be higher based on the configuration of the mutations and if that’s the case and latency isn’t extended significantly over delta – omicron may readily replace delta as the dominant variant in most countries. Early reports from South Africa also suggest transmission will be high.
While it will likely be days or weeks before omicron’s potential virulence and transmissibility can be better appreciated, the configuration of mutations – highly conserved within the spike protein itself – tells us that there’s a high likelihood that existing injections will be even less effective than on delta. This view is confirmed by none other than Dr Anthony Fauci, as well as others, such as Dr Samiran Panda who heads the Epidemiology & Communicable Diseases Division of the Indian Council of Medical Research (ICMR).
The pace at which the new variant has been used by politicians to push first-generation injections on the public, along with everything else we know about the host-pathogen-injection interaction, is breathtaking given the uncertainties involved with this policy. They know, for example, these injections were designed to elicit antibodies that are highly specific to the original Wuhan strain’s spike protein and they also know the configuration differs substantially to that of the omicron variant.
While the public is being told they should boost their immune system with the existing injections, they're not being told that there could be grave costs to this, like damaging innate immunity, inducing more severe reactions to disease, enhancing transmission or exposing countless people to unnecessary, potentially debilitating or life-threatening adverse reactions. Pfizer has already announced it’s working on making new injections built specifically for Omicron and these might be 100 days away. The immediate decision to foist the old injections on the public to ‘boost’ immunity with what are probably even more weakly neutralising antibodies at best is clearly based on political or economic, not medical, expedience.
Where did Omicron come from?
The world’s media is typically claiming Botswana or South Africa as the country in which Omicron was first detected. It is true that the largest numbers of cases have been found there, as evidenced by the country submission count on the GISAID variant tracker, as seen in Table 2.
Table 2. Most recent reported occurrences of omicron variant in different countries.
|
Country |
Total #GR/484A (B.1.1.529) |
#GR/484A (B.1.1.529) in past 4 weeks |
%GR/484A (B.1.1.529) in past 4 weeks |
|
South Africa |
171 |
171 |
71 |
|
Botswana |
19 |
19 |
22.4 |
|
Portugal |
13 |
13 |
1.3 |
|
Netherlands |
12 |
0 |
0 |
|
United Kingdom |
9 |
9 |
0 |
|
Australia |
6 |
6 |
0.4 |
|
Germany |
5 |
5 |
0.1 |
|
Hong Kong |
5 |
5 |
20.8 |
|
Italy |
4 |
4 |
0.1 |
|
Austria |
4 |
4 |
4 |
|
Canada |
2 |
2 |
0.3 |
|
Brazil |
2 |
2 |
0.3 |
|
Japan |
2 |
2 |
4.8 |
|
Sweden |
1 |
1 |
0 |
|
Belgium |
1 |
1 |
0 |
|
Reunion |
1 |
1 |
1.2 |
|
Israel |
1 |
1 |
0 |
|
Spain |
1 |
1 |
0.1 |
|
Czech Republic |
1 |
1 |
0.2 |
Source: GISAID. Downloaded 1 Dec 2021.
But it’s also clear, from the GISAID records, that neither Botswana nor South Africa were the countries in which the earliest detection of omicron (variant B.1.1.529) occurred. Collections in Sweden, Israel, Reunion and the UK all appear to precede those from Botswana and South Africa. Check out the table from GISAID below, which is in reverse chronological order.
Table 3. Country submission count to GISAID as of 1 December 2021
|
Country |
Strain Name |
Collection Date |
|
Italy |
hCoV-19/Italy/CAM-COLLI-COTUGNO-A10117/2021 |
28/11/2021 |
|
Japan |
hCoV-19/Japan/IC-2278/2021 |
28/11/2021 |
|
Spain |
hCoV-19/Spain/MD-HGUGM-5821169/2021 |
28/11/2021 |
|
Australia |
hCoV-19/Australia/NSW-ICPMR-14637/2021 |
28/11/2021 |
|
Austria |
hCoV-19/Austria/MUIV-0231/2021 |
28/11/2021 |
|
Portugal |
hCoV-19/Portugal/PT21719/2021 |
27/11/2021 |
|
Germany |
hCoV-19/Germany/BY-MVP-000009711/2021 |
27/11/2021 |
|
Czech Republic |
hCoV-19/Czech Republic/KNL_2021-110119140/2021 |
26/11/2021 |
|
Hong Kong |
hCoV-19/Hong Kong/VM21045834/2021 |
26/11/2021 |
|
Brazil |
hCoV-19/Brazil/SP-HIAE-ID989/2021 |
25/11/2021 |
|
South Africa |
hCoV-19/South Africa/Tygerberg_3072/2021 |
25/11/2021 |
|
Belgium |
hCoV-19/Belgium/rega-20174/2021 |
24/11/2021 |
|
Canada |
hCoV-19/Canada/ON-NML-249359/2021 |
23/11/2021 |
|
Botswana |
hCoV-19/Botswana/R43B70_BHP_4021000195/2021 |
23/11/2021 |
|
United Kingdom |
hCoV-19/Scotland/QEUH-2BA64B4/2021 |
23/11/2021 |
|
Reunion |
hCoV-19/Reunion/PIMIT_Om1/2021 |
22/11/2021 |
|
Israel |
hCoV-19/Israel/SMC-7022800/2021 |
20/11/2021 |
|
Sweden |
hCoV-19/Sweden/10190023/2021 | 19/11/2021 |
Source: GISAID. Downloaded 1 Dec 2021.
Today we hear that a sample collected in October in Nigeria from an “incoming international traveller” was positive for omicron.
No doubt a lot more will be revealed in time. For us, currently available information means the jury is absolutely out as to whether omicron originated in Africa at all. The origins might well have been a traveller from a highly vaccinated country that imported it to Africa. Dr Masupu of the Presidential Covid-19 Task Force of the Botswana Government confirmed that the 4 university students known by the task force to be infected with omicron were all fully vaccinated.
We also know that blaming omicron on Africa makes sense if there is to be mounting pressure to vaccinate the world’s least vaccinated continent, that also has by far the fewest issues with covid-19 (see Fig. 1). Much of Africa – it seems – doesn’t want to play ball.
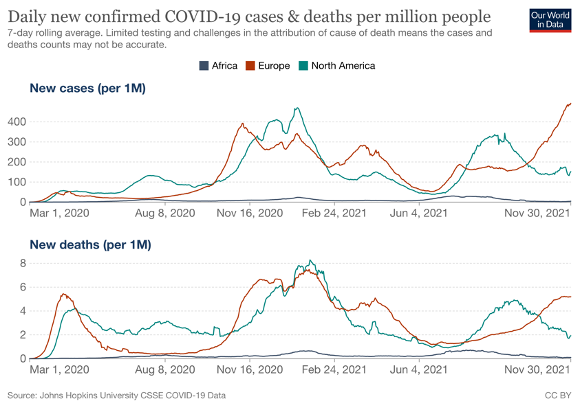
Figure 1. Daily new confirmed covid-19 cases and deaths per million people in 3 continents: Africa, Europe and North America. Source: Our World in Data
What we also know is just after South Africa announced it didn’t want to accept more covid injections from Pfizer or Johnson & Johnson, the omicron alarm bell was sounded. Coincidence?
Possible consequences of using boosters in an Omicron wave
What we have witnessed since early 2021 when covid jabs were rolled out across the industrialised world is a gradual loss of synchronicity in the injection efforts. Different countries had different uptakes, the speed of roll out across successively younger age groups, hesitancy and refusal varied country to country and sometimes even region to region. All of that loss of synchronicity actually reduces selection pressure – as does having big reservoirs of unvaccinated young people with lively innate immune systems, like in much of the African continent.
Omicron will re-synchronise the injection campaigns. Vast numbers of people will get a top up of the first generation jab, only to be hit yet again when the ‘must-have’ omicron-specific jab rolls off the production line probably in under 4 months. More synchronisation means that more intense selection pressure will be applied to the spike protein of omicron, and more replication will occur as the antibodies generated by the injections will not effectively block infection. This creates the vicious circle that Geert Vanden Bossche has described that we have been caught in already for a year with ever greater risk of more dangerous and more infective mutants being generated.
Higher frequency of exposure also means more insults to the immune system and that means more damage to the innate immunity of our species – our primary weapon against a mutating pathogen. The conditions are set for escalating risks of antibody-dependent enhancement (ADE) of disease when injected people are exposed to disease, as well as an ever greater toll of adverse events and deaths mediated by autoimmunity, inflammation, neurological and cardiac issues.
The consequences of a bad outcome for humanity are scarcely worth considering – and it seems that’s why the politicians, ushered along by a vaccine/biotech/pharma industry with an insatiable appetite for maximising profitability while avoiding any liability for any damages caused – are going with it.
If vaccine passports and digital IDs for everyone on the planet, as precursors to a new digital currency and the merging of man and machine (transhumanism), are elements of the real end-game, it makes even more sense why global leaders are so up for it. Just don’t be fooled that this is about a virus, medicine or science.
Ominous omicron
Just as the earlier unscientifically-based decisions to lockdown, mask up and socially isolate populations at the beginning of this pandemic was an ominous signal of the authoritarianism and suppression that was to come, omicron’s arrival is just as ominous.
Once again, it’s not the virus we should primarily worry about if we can help our immune systems to be the best versions of themselves, and if we can access early treatments that are variant agnostic. It is the reaction of governments, health authorities, politicians and business leaders who seem hell bent on continuing this failing, ever more risky endeavour of installing synthetic instructions into our bodies, the consequences of which will not be well known to the public for some years. Bear in mind that the US Food & Drug Administration asked a federal judge to make the American public wait until 2076 (yes, 55 years!) before all of the data on Pfizer’s ‘genetic vaccine’ it relied on for approvals are made public. The great news is the judge has just forced Pfizer to release the documents incrementally — the first lot being something of a revelation in terms of the adverse event profile. More on that next week.
Without our trust, one wonders if ‘they’ are beginning to understand why so many of us around the world are conscientious objectors?
Please Digest. Share. Educate.
More information from our partner, the World Council for Health
>>> World Council for Health statement on omicron
>>> World Council for Health Early Covid-19 Treatment guidelines
#enoughmovement #enough




Comments
your voice counts
02 December 2021 at 10:36 am
There has been absolutely NO mention of using a really potent anti-viral natural supplement - Monolaurin by anyone during the pandemic. It is really worth researching this. I have been using it daily with my sons, husband and myself and also my clients throughout the pandemic as part of an immune-boosting programme.
Fleur Brown
Nutritional Therapist
02 December 2021 at 10:44 am
Bioactive monolaurin as an antimicrobial and its potential to improve the immune system and against covid-19: A review
Anonymous.
Food Research ; 4(6):2355-2365, 2020.
Article in English | Scopus | ID: covidwho-951340
ABSTRACT
Monolaurin is monoacylglycerol which is a bioactive lipid since it can affect the human biological systems. This review discusses the bioactive properties of monolaurin, especially its role as an antibacterial, immune system enhancement, and its ability as an antiviral so that it has the potential to fight against various viral attacks. Monolaurin can act as an antibacterial in inhibiting the growth of several pathogenic bacteria, especially gram-positive bacteria. Monolaurin is known to be able to enhance the immune system through modulation of various immune systems, controlling pro-inflammatory cytokines, activating and attracting leukocytes to the site of infection. Monolaurin can also act as an antiviral, especially against enveloped viruses, such as Maedi-visna virus, vesicular stomatitis, herpes simplex-1, measles, HIV, cytomegalovirus, influenza, and corona. Monolaurin inhibits the virus through the mechanism of the disintegration of the viral membrane, prevents binding of the viral protein to the host-cell membrane, inhibits the process of assembling the viral RNA, and the process of virus maturation in the replication cycle. Therefore monolaurin has the potential for human consumption to boost the immune system and ward off various virus attacks, including severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is the cause of COVID-19 which became a pandemic in the world. © 2020 The Authors.
02 December 2021 at 10:56 am
We can discuss the pros and cons of booster shots but that is no help to those of use who are being forced into accepting them or we have to isolate ourselves from all normal social contact. As an elderly woman living in France who suffered side effects for nearly 5 months from a second Covid shot and who now has continuous sub-clinical shingles I am being forced to accept the booster otherwise my health pass will be negated and thus my social contacts restricted. The booster has to be administered by the 15th December nicely timed to restrict most Christmas socialisations and a real blackmail move by a government indulging in a knee jerk reaction. My doctor is not authorised to write any exemption..I am still thinking what to do but I guess I will knuckle under and reluctantly comply. This will be recorded as an acceptance statistically ie positive support for the booster.
02 December 2021 at 3:41 pm
Hello Mary
Thank you for taking the time to comment and let us know what's happening in France. We're sorry to hear how you're being treated currently and that the adverse reaction you've suffered is being ignored. The way people around the world are being treated currently is criminal. To hear that your doctor is not authorised to give you an exemption is truly shocking.
In the event you do 'knuckle under' we hope you aren't harmed any further. If you need a friendly voice we're at the end of the phone, please feel free to call and have a chat.
Warm wishes
Melissa
02 December 2021 at 5:06 pm
Thank you Melissa for your supportive reply and thank you for your offer of a chat. Depending on the results of my appointment with my doctor on Tuesday I may well contact you. Apparently it might difficult to get a booster shot before the 15th. Be interesting to see how that problem will be dealt with!
Regards and thanks
Mary
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences