

Content Sections
By Rob Verkerk PhD, ANH founder, executive & scientific director
TOPLINE
- As negotiating time over the International Health Regulations and 'pandemic treaty' runs out, misinformation and disinformation abounds on all sides
- Fundamental to the proposal is the notion of moving the locus of control from the individual, side-stepping the physician, and putting faceless, unelected and unaccountable bureaucrats in charge of health during times of international public health emergencies and pandemics
- The WHO plan is claimed to be all about equity and fairness, but it runs contrary to many fundamental human rights and long-standing principles of medical ethics
- The current negotiations are fundamentally undemocratic and most elected representatives who have spoken out have found themselves isolated and branded as conspiracy theorists.
“Every human being of adult years and sound mind has a right to determine what shall be done with his own body”— Justice Benjamin N. Cardozo, 1914 (Cardozo B. Basic right to consent to medical care − Schlendorff vs the Society of the New York Hospital, 211 NY 125 105 NE 92 1914 LEXUS 1028 [1914])
Once upon a time
In a Supreme Court decision in New York back in 1914, Justice Cardozo set one of the most important foundation stones for modern medical ethics, the principle of autonomy in healthcare decision-making. This wasn’t a new idea, it is one enshrined in many ancient texts, such as the Vedic texts of India and the Nei Ching of Chinese Medicine. The importance of this ethical principle in healthcare was reinforced more recently by German philosopher Immanuel Kant (1724-1804) and the English philosopher John Stuart Mill (1806-1873) before being firmly set by Tom Beauchamp and James Childress in 1979.
Autonomy: ready for sacrifice?
In a modern context, building on the views of Kant, autonomy means that all persons have intrinsic and unconditional worth, and therefore, should have the power to make rational decisions and moral choices, and each should be allowed to exercise his or her capacity for self-determination.”
But autonomy as a medical ethics principle is now under unprecedented threat, globally. The source of that threat is the most powerful health authority in our increasingly globalised world; the Swiss-based, unaccountable, international non-profit organisation known as the World Health Organization (WHO). The scale and nature of the threat will become apparent in the coming months, during the lead up to the voting by 196 countries at the next meeting of the World Health Assembly in Geneva between May 27 and June 1. The votes will determine how countries should respond in the event of future pandemics or global health emergencies, circumstances we are told over and over again we should come to expect more often than in the past.
The global plan that is being driven by the WHO and its leading funders, the top six, in descending order of contribution, being Germany, the Bill & Melinda Gates Foundation, the USA, the European Commission, GAVI Alliance, and the UK. If the WHO declares another pandemic or ‘public health emergency of international concern’ (PHEIC), something it can do unilaterally on the basis of very limited criteria, the plan, if enacted, will involve an international response, and consequent national responses, that run quite differently to our recent experience of the COVID-19 pandemic between March 2020 and May 2023. It should be noted that a single individual, namely the director-general of the WHO, currently Dr Tedros Adhanom Ghebreyesus, has the sole power to declare a PHEIC, and this one individual is unelected by the people, unaccountable and has immunity from prosecution by virtue of ‘diplomatic immunity’.
If you thought the COVID-19 pandemic response by governments, health authorities, corporations and the media last time around was too heavy-handed, too top-down or too authoritarian, don’t imagine the next one will be more even handed. Conversely, if you thought the response wasn’t sufficiently robust, that lockdowns weren’t forceful or long enough, that there wasn’t enough testing, tracking or surveillance, that mask wearing wasn’t mandated sufficiently, that people were given too much leeway to travel, that previously untrialled, novel genetic vaccines weren’t rolled out quick enough or in sufficient number, or that those who exercised their right of refusal weren’t penalised sufficiently, well…you’re going to be thrilled with what’s in the pipeline.
The next time round, the pandemic response by nations and international authorities will almost certainly be more authoritarian and control will be much more centralised, masterminded from the WHO headquarters in Geneva. Countries will have a binding responsibility to comply with their masters at the WHO, and rich countries will have to gift lots of their hard-won money and healthcare products to poorer countries. All in the name of health equity, very much the buzz word of the current negotiations. This is at least the vision of many of the most powerful world leaders – on both the political and corporate stage.
And here’s the thing, to make this happen, it means ditching or, at least, severely limiting, individual decision-making of health, the fundamental tenets of ‘autonomy’, one of four foundational pillars of modern medical ethics. It also means kissing goodbye to the joint decision-making that has long existed between physicians and the public, and passing that responsibility to faceless institutions and authorities who have zero understanding of your health status, your resilience or sensitivities, your health needs, or your circumstances.
Moving the locus of control over health by taking health responsibility away from the individual, bypassing primary care physicians or other community-based health practitioners, and passing it to a faceless bureaucracy should be an anathema. At least to the many thousands of us who have been working tirelessly towards increasing people’s access to personalised and individualised systems of health that are tailored to the needs, circumstances and environment of each person.
The two key negotiating tables
The detail of how the global pandemic response is expected to be achieved, and exactly what mechanisms and processes will be brought to bear on us mere mortals in the event of the next global public health emergency, is currently unknown. That’s because it’s all still on the negotiating table, and negotiations are at fever pitch right now, with significant parts of it going on behind closed doors and most of it being unreported by the mainstream media.
There are, in fact, two negotiating tables involved, but both are controlled by the very organisation that is primed to become the supreme power broker in the event of the next health emergency, the WHO.
Let’s take a quick look at these two negotiating tables, and offer you their respective hyperlinks so you can do your own digging should this appeal. One is the Working Group on Amendments to the International Health Regulations (WGIHR) that is currently dealing with over 300 amendments to the existing International Health Regulations of 2005, many of which strengthen the power of the WHO and weaken national sovereignty in the event of a PHEIC. The other is the Intergovernmental Negotiating Body (INB) that is responsible for drafting and negotiating the so-called ‘pandemic treaty’ (increasingly referred to as an ‘accord’ so escapes the definition or ‘treaty’ and can side-step parliamentary or congressional approval), that is an “international instrument under the Constitution of the World Health Organization [that intends] to strengthen pandemic prevention, preparedness and response.”
The WHO likes to claim that the nearly 200 countries that are members of the WHO are running the show in each of these two negotiations. This view is meant to make us feel that the process is democratic, the it is the will of the people. But that’s a pipe dream. There are a few powerful players, like the USA, Germany, the unelected European Commission and the UK, and these have the ability to coerce other countries who will likely face penalties if they don’t play by the emerging global rules. There are many ways smaller and less developed countries can be forced to play by the rules. Two important devices include the building or breaking of trading relationships, or the conditions under which international loans, such as those from the International Monetary Fund, are paid off, deferred or forgotten.
Out of sight, out of mind
The problem with negotiations of the type that the WGIHR and INB are undertaking is that they’re entirely undemocratic in the true sense of the word. The people or electorates in the 196 countries involved, including 194 WHO ‘member states’, don’t get to have any kind of say. That’s because those engaged in the negotiations are unelected bureaucrats ‘doing a job’ and there’s no direct line of communication between elected representatives and these bureaucrats.
In many countries, a few, diligent elected representatives have tried raising their concerns in their own parliaments or assemblies. But we see a common pattern. Very few other representatives attend the hearings, and there is almost a whitewash on mainstream press coverage.
Take the British member of Parliament, Andrew Bridgen, for example. He has raised more than once, to an almost empty ‘house’, the very concerns over the IHR amendments and ‘pandemic treaty’ that we have been vocal about previously (such as here and here). That includes the removal of the term “non-binding” from Article 1, and insertion of the phrase in Article 13A that says “Member States [will] undertake to follow WHO recommendations.”
But it’s even worse than that. The vast majority of the public aren’t even aware these negotiations are going on or what’s at stake. Why? Because concerns over the outcomes of the negotiations are just not being reported by the mainstream media.
Below you’ll hear Congressman Andy Biggs (R-NJ) raising awareness in Congress of his bill that pulls the US out of the WHO.
Another congressman, Chris Smith (R-NJ), hosted a press conference on Monday (February 5) about the ‘pandemic accord’, with invited experts that was barely reported. Included in discussion was the lack of transparency, the backroom negotiations, WHO overreach, infringement on US sovereignty, unknown financial obligations for US taxpayers, threats to intellectual property rights, free speech, funding for abortion, and how it will benefit China at the expense of the US. You can watch the press conference below.
None of these presentations by elected representatives makes the mainstream press. The coverage in the New York Times is much more typical of how the mainstream media has been covering the IHR and ‘pandemic treaty’. By example, type in the phrase ‘International Health Regulations’ into the search box of the New York Times and you’ll find no coverage about the negotiations. You simply find articles that endorse the principle of the WHO running the show, such as this one published the day after the WHO declared the pandemic on March 12, 2020, with the title “The World Has a Plan to Fight Coronavirus. Most Countries Are Not Using it.”
Type ‘pandemic treaty’ into the UK’s The Guardian website and you’ll find stories, such as this one, “Can a WHO pandemic treaty help poorer nations in future outbreaks?” (August 10, 2023), that talks to the desperate need by poorer countries to receive vaccines in the event of a pandemic. This is odd, given many of the poorest countries didn’t have either much of a need nor an interest in getting their hands on COVID-19 vaccines last time around.
This kind of reporting underpins the public relations exercise the WHO and its big contributors, including vaccine interests like the Gates Foundation and the GAVI Alliance, are promulgating in order to give the WHO more muscle, to make it top dog in the hierarchy of global control of health — and more.
The WHO muscle-building plan
Ostensibly, the goals of the WHO are worthy, “to promote, provide and protect health and wellbeing for all people, everywhere.” These are the first three Ps that Tedros spoke of in his opening remarks to the 154th session of the Executive Board of the WHO on January 22, 2024. (In case you wondered, the other two Ps are Power and Perform, concepts that can seem scary in the hands of an unaccountable body).
The WHO muscle-building plan can’t happen overnight as it inevitably needs to follow the deceptive and insidious, well trodden approach of ‘boiling the frog slowly’ (in the hope everyone will get used to the direction of travel and succumb to it). The manifesto is already scripted in the WHO’s upcoming 14th General Programme of Work (GPW 14) (see Fig. 1) that’s intimately connected to the UN’s Sustainable Development Goals. The WHO has found a way of putting health right at the centre of what it calls the ‘converging crises’ of climate, food, energy and geopolitics.
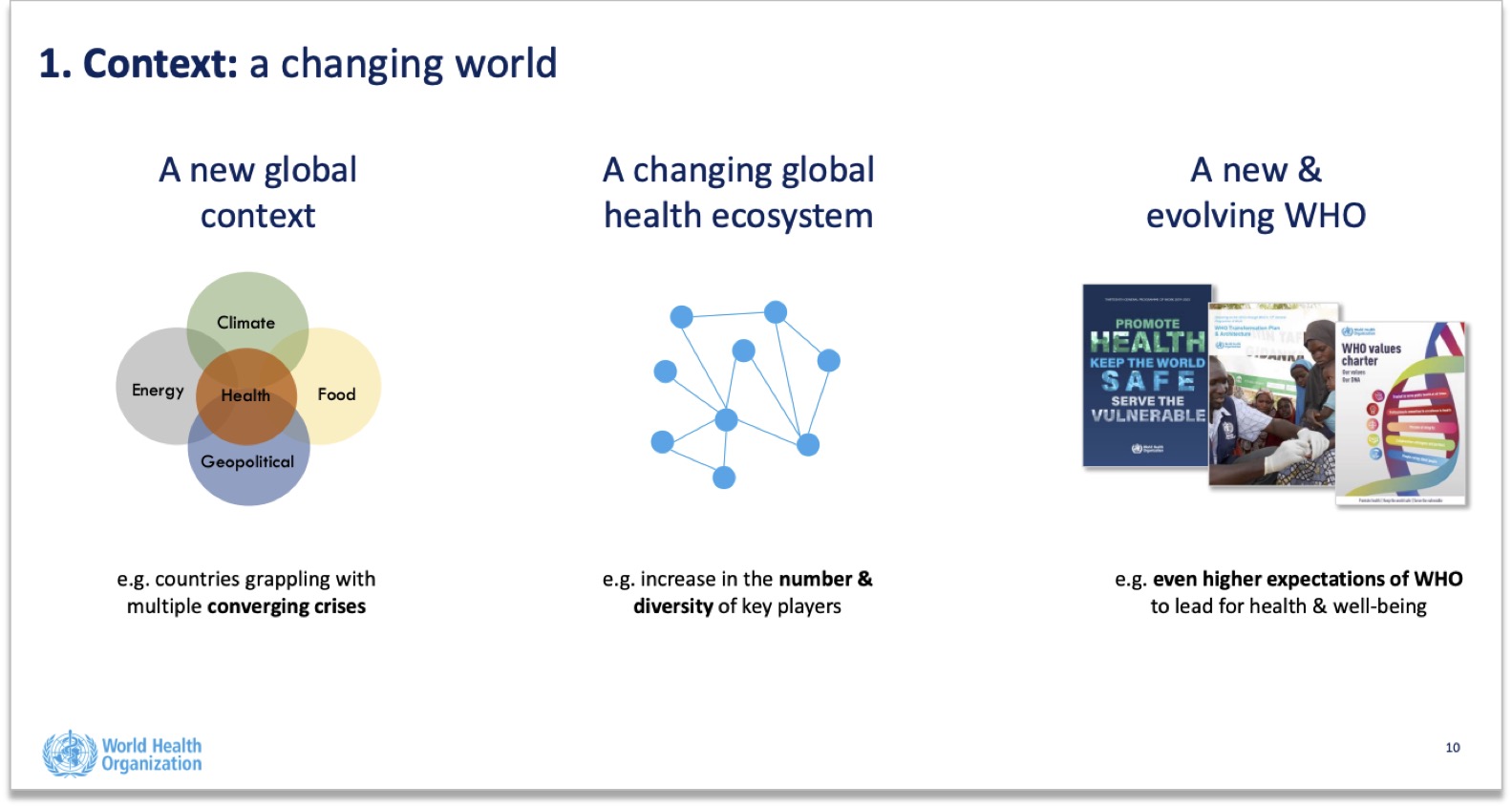
Figure 1. Extract from WHO “Towards GPW14 (2020-2028)” document, published July 2023. Source: WHO.
If that wasn’t enough, the health of humans is now expected to be better managed by linking it directly to that of domestic and wild animals, plants and the wider environment through One Health. This is described as a “unifying approach” that “aims to sustainably balance and optimize the health of people, animals and ecosystems.” With unbridled confidence, the WHO declares that “One Health can help to address the full spectrum of disease control – from prevention to detection, preparedness, response and management – and contribute to global health security.” It’s a nice concept in that it recognises the human interconnection with nature, but it’s not so nice if it’s all about installing top-down control over every facet of human, animal and planetary health, a concept that has been likened by those carrying the conspiracy theory tag on their foreheads as akin to global governance.
One significant problem with this globalised approach is that there’s no evidence it works. The authorities and most academics failed to see whether regionalisation or individualisation of approaches that included keeping schools open for children, avoiding use of masks or receiving any or multiple genetic vaccines during the height of the COVID-19 pandemic worked better than one-size fits all, globally controlled approaches.
As it happens, many of us in natural health circles did experience just how effectively individualised approaches, ones that ran diametrically against the WHO recommendations, worked. I led a team who evaluated data collated by a UK-based non-profit called the Control Group, the works being subsequently published in the International Journal of Vaccine Theory, Practice, and Research, a journal specifically launched given most journals refusal to publish science that ran contrary to the narrative.
Regardless of push-back, a process continues to gather momentum that is in no way being supported by the majority of people on the planet, one that is attempting to centralise control over health, rather than individualising it. This is being done without evidence of its value or ability to resolve our ever growing health challenges.
The WHO has also scripted its plan in its updated document, “WHO benchmarks for strengthening health emergency capacities”, as the title suggests, to show how different countries’ health emergency capacities can be benchmarked so they can get behind the WHO’s plan for health equity (read: authoritarian control). Nowhere within the document is there any mention of how people’s nutritional or immune status might be a useful benchmark of a countries capacity to withstand new infections. ‘Optimum vaccine coverage’, by contrast, gets a big mention as a key benchmark.
Taken altogether, it is clear that the WHO is lock, stock and barrel sold on the idea that vaccines should be by far the most important medical intervention in the event of new pandemic, and it’s also clear that the WHO and its allies are desperately keen to make sure coverage is as complete as possible. This rationale is astonishing in view of the facts that COVID-19 genetic vaccines failed to stop transmission, have driven (and continue to drive) the production of immune escape variants, caused more severe disease in those who took more than 2 shots, and caused extensive harms (e.g. OpenVAERS data). We all understand how higher coverage could be made to work, such as through mandates, coercion or withdrawing freedoms from those who choose to avoid. We also recognise that elevated surveillance and so-called ‘vaccine passports’ may well be forced through in the name of ‘global health security’. Mention any of this to anyone who’s sold on the plan, and you’ll be told you’re a conspiracy theorist. Just saying.
Dissenters are full of "fake news, lies, and conspiracy theories", says Tedros
And guess what Dr Tedros is saying about it all? Apparently us dissenters have it badly wrong, that the proposed “binding” agreements that countries will vote on in May will all be brought to bear under national laws so the WHO can't be accused of any power grab. At his January 22 opening remarks at the informal briefing on the INB and WGIHR, Tedros said:
“The INB and the IHR working group are operating amid a torrent of fake news, lies, and conspiracy theories. There arethose who claim that the pandemic agreement and IHR will cede sovereignty to WHO and give the WHO Secretariat the power to impose lockdowns or vaccine mandates on countries. You know this is fake news, lies, and conspiracy theories.”
- Director-General of the WHO, Dr Tedros Adhanom Ghebreyesus, January 22, 2024.
[Transcript available on WHO website].
The nub of the discrepancy in view boils down to who (pun 1) calls the shots and who (pun 2) maintains or delegates authority over which issues during a declared international health emergency. The WHO says the process is WHO member state-led therefore the WHO does not control it. Opponents of the process, ourselves included, say by making the International Health Regulations binding (as proposed by amendment to Article 1 on Definitions), international law will have supremacy over national laws. If that law places control during health emergencies into the hands of the WHO, nations will have elected to give up their powers on related matters, delegating them upwards to the WHO, justified presumably because these countries deem the WHO to be the most expert and powerful entity in the event of a global pandemic response. In practice, this means, at least while an international public health emergency is active, nation states will have effectively ceded their sovereignty to the WHO. While this seems like splitting hairs, what matters most is the effect, not the mechanism, of the process.
What next?
Today marks the last day of the 7th (and penultimate) meeting of the WGIHR and we eagerly await outcomes, the summary of which will be delivered by public webcast.
Prior to the vote and adoption of the IHR amendments at the 77th meeting of the WHA at the end of May, it will take a further 18 months for these amendments to come into effect. This time may provide additional opportunities for more pushback if the outcomes of the current negotiations and the May vote are unfavourable for individual health and national sovereignty.
There is no doubt that public pressure and political resistance is slowing down and complicating the plan to create a “safer and fairer world”, one that massively disempowers the role of the physician and pretty much relegates the ever-more diluted, 4 guiding principles of contemporary medical ethics, namely autonomy, beneficence (doing good), maleficence (minimising harm) and justice, to the trash can.
We will continue to stay on top of developments in these murky supranational negotiations and we'll keep providing our readers and subscribers with a view from the perspective of those who still value Justice Cardozo’s 110-year-old perspective, that “Every human being of adult years and sound mind has a right to determine what shall be done with his own body.”
As Canadian-American psychotherapist Nathaniel Branden famously said, “The first step towards change is awareness. The second step is acceptance.”
Please circulate this article widely to your networks to improve awareness of these issues that are not being reported by the mainstream media, and help beat the censors.
>>> Visit covidzone.org for our complete curated covid content of the coronavirus crisis
>>> If you’re not already signed up for the ANH International weekly newsletter, sign up for free now using the SUBSCRIBE button at the top of our website – or better still – become a Pathfinder member and join the ANH-Intl tribe to enjoy benefits unique to our members.
>> Feel free to republish - just follow our Alliance for Natural Health International Re-publishing Guidelines
>>> Return to ANH International homepage



Comments
your voice counts
10 February 2024 at 1:21 am
God help us. Thank you to ANH and others including lawyer Philip Krause for bring the next scam to our attention in detail that can be shared. We have to share widely to ensure our freedoms. Once lost we are done for.
10 February 2024 at 8:06 am
Thank you for taking the time to read the article Jennifer and for helping to spread the word about the machinations of the WHO and other players that would take our freedoms away from us.
14 February 2024 at 2:08 pm
Thank you so much ANH for yet more detailed news and information, I give you a standing ovation for all you are doing for the good of our health.
15 February 2024 at 7:41 am
Thanks so much Janet and for all your support as well.
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences