
By Rob Verkerk PhD, founder, scientific and executive director
For all of you who’ve been diligently monitoring the various Covid trackers, you’ll have noticed some very divergent patterns in terms of numbers of confirmed cases, new cases and trends. China appears to have the disease completely under control, although the accuracy of some of the data emerging from China has been challenged and a resurgence of the disease could easily occur in the future as it is highly unlikely that most of China’s 1.4 billion population has so far acquired immunity.
-
Find related articles, information and videos in our Covid Zone
Others like South Korea, Australia and Norway, all with relatively small numbers of confirmed cases, are experiencing a flattening of their curves, while many more, such as Spain, Germany, Italy, Iran and Switzerland, are witnessing just the beginning of such a trend (Figure 1).
More disconcerting is of course the many countries that have yet to see any appreciable flattening. That includes populous countries like the USA, UK, Netherlands, Turkey, Brazil – along with many others (Figure 1). But with all this talk by governments and their scientific advisors of the need to ‘flatten the curve’, let’s remember you’re looking at the cumulative total of confirmed cases which requires there to be zero new cases to see a flat line, like China’s currently (Figure 1).
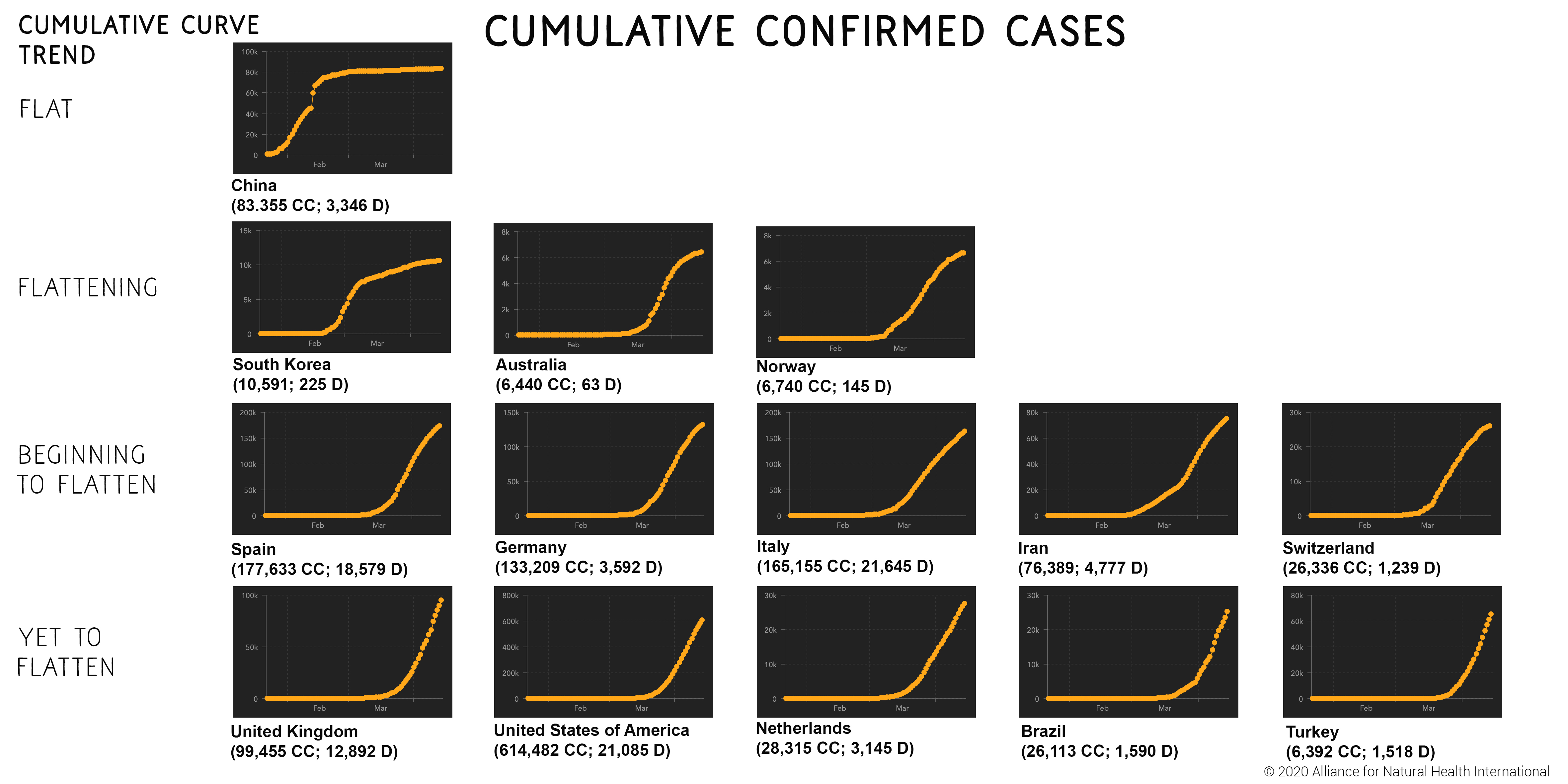
FIGURE 1. Different trends in the curves for confirmed cases among selected countries. Where CC = confirmed cases; D = deaths, based on data on 15 April 2020 from Johns Hopkins University of Medicine, Coronavirus Resource Center.
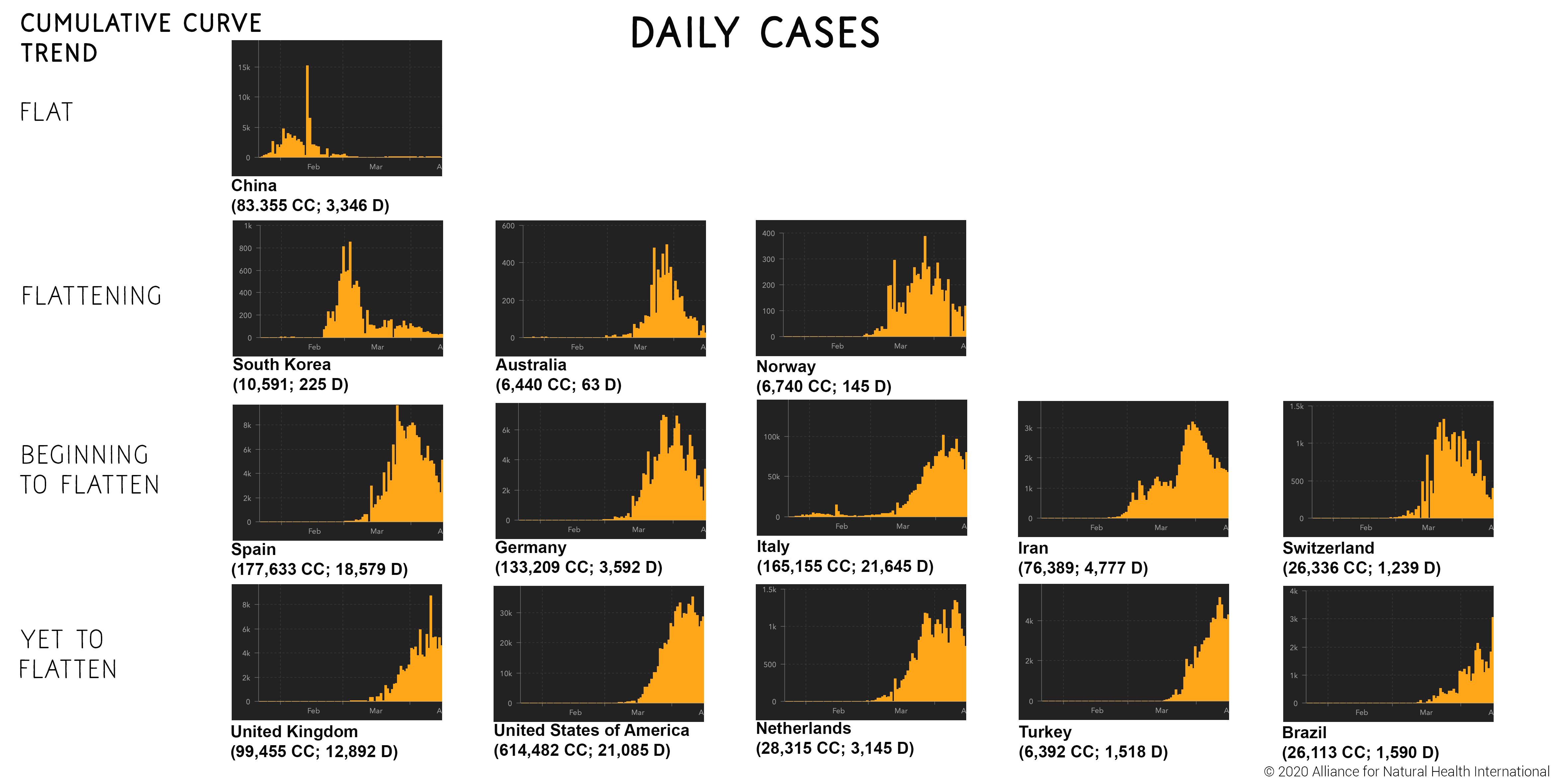
FIGURE 2. Different trends in the curves for confirmed cases among selected countries. Where CC = confirmed cases; D = deaths, based on data on 15 April 2020 from Johns Hopkins University of Medicine, Coronavirus Resource Center.
You get a better idea of what’s happening at the most recent point in time with the overall epidemiology or viral spread in a given country by looking at the trends in daily occurrence of new cases. So when you look again at the same selected countries shown in Figure 1, you’ll see that even those countries that appear not yet to have flattened the curve, like the UK and US, appear to be over the peak in number of new cases (Figure 2).
There are also many countries that have suffered very little in the way of Covid-related incidence and deaths – many of these being densely populated in warmer or tropical climates, such as Sierra Leone that was hit so hard by Ebola.
This begs several questions, such as: what caused infections rates to slow so markedly or for infections to hardly take off at all? Have the lockdowns and social distancing been the driving force behind declining new cases, or are other factors at play? And just how important are environmental factors?
The reality is that the scientific community does not have a solid view on these questions. But what is beginning to emerge is that social distancing and lockdowns might increase the risk of a rebound – and provide a stronger argument for the perceived need for a vaccine, for which there were 115 candidates in development as of 8 April.
Given the unique features of this disease, we get our most valuable lessons from looking at data for Covid-19, not other respiratory infections. Here, Japan and South Korea provide two of the best examples because the first infection surge in those countries appears to be well and truly over.
Flattening the curve prolongs the disease
Knut Wittkowski PhD, a renowned scientist and epidemiologist – previously the head of the Department of Biostatistics, Epidemiology, and Research Design at The Rockefeller University, New York – and currently CEO of Asdera LLC that’s focused on discovery of novel treatment for complex diseases, has a particularly interesting take on it.
You can read the paper he’s just published in MedRxIV or watch an interview of him below.
Among the key take homes are:
- The natural history of new infections such as the SARS-CoV-2 virus infection that causes Covid-19 means peak infection will occur quickly and in most countries would likely be over inside 90 days once naturally-acquired herd immunity through the majority of the population has been achieved – without national, untargeted lockdowns and social distancing
- Wittkowski qualifies this time frame in the following way, stating, “...that the SARS-CoV-2 data…also suggest that it takes at least a month from the first case entering the country (typically followed by others) for the epidemic to be detected, about three weeks for the number of cases to peak and a month for the epidemic to 'resolve'"
- This might result in 2% mortality among those infected, that would be able to be handled by a slight and temporary ramping up of critical care facilities
- Evidence from China and South Korea shows that the downturn in new cases started at least two weeks before lockdowns were enforced. This would suggest that the decline was a response to increased naturally-acquired immunity and not the lockdowns
- Lockdowns applied too early (e.g. many European countries, many states in the USA) with the intention of ‘flattening the curve’, well before peak infections are expected (e.g. UK, USA), prolong the infection and increase the likelihood of rebound in the future
- Wittkowski’s real data informed model suggests that without lockdowns and social distancing, but including efforts to shield vulnerable and elderly populations, the Covid-19 epidemic would be over by mid-April (now) in Europe and beginning of May in the USA
- Wittkowski also upholds that it is likely that there is more than one strain of SARS-CoV-2 circulating, the second having considerably lower infectivity and lethality.
Is the cure worse than the disease?
This is the question that is on many of our minds. It’s being increasingly asked by the public and even the media. Governments seem hazy in their responses and for many it seems that primary strategy is ‘let’s make it up as we go along’.
It’s always easier to be critical in hindsight, but a few home truths are becoming increasingly apparent:
- Many governments have failed disastrously in the provision of adequate personal protective equipment (PPE) to those who need it most in the frontlines and this has created unnecessary spread of infection, sickness and death
- Quality control on antigen (swab) tests for presence of the virus and antibody (blood) tests for existing immunity has been incredibly badly managed in countries like the UK and USA. Either there has not been enough tests available or many have been inaccurate, delivering a high proportion of false positives or negatives
- 50% survival rate in critical care, such as the UK intensive care units (ICUs) is both unacceptable and unnecessary
- Very simplistic government messages aimed at maintaining lockdown have underestimated the public and failed to empower citizens to take responsibility for their health and improve the resilience of their immune systems, the single most important defence system each one of us has if infected by the virus
- The absence of clear exit strategies from lockdowns by some governments, along with increased police enforcement, set the seeds for social unrest and uprising given the questionable net risk/benefit of national lockdowns and their huge direct and indirect, social, economic, and even health, consequences.
What should the Covid smorgasboard look like?
Many of us are becoming increasingly frustrated by the make-it-up-as-you-go-along strategy of governments.
There are a huge variety of things we could all be doing, and removing civil liberties and freedoms and imposing untargeted widescale lockdowns is only one of the options.
We’ve created a list below of a much wider range of options that we believe the public and parliaments, at least in so-called democratic countries, should have been engaged in exploring or trialling.
They are as follows:
- Social distancing
- National lockdown (domestic and commercial, non-essential services)
- Selective lockdown (e.g. only vulnerable groups)
- Provision of effective PPE to healthcare and essential service workers in high exposure/high risk situations
- Antigen testing and confinement of infected individuals – from frontline healthcare workers to general public
- Antibody testing and resumption of normal activities of immune individuals – from frontline healthcare workers to general public
- Widescale antigen and antibody testing with relevant actions depending on results – from frontline healthcare workers to general public
- Antigen testing, combined with contact tracing [particularly difficult with respiratory viruses given extent of airborne transmission]
- Effective approaches to immunity enhancement e.g. nutritional, therapeutic
- Improved effectiveness of critical care approach and therapeutics (e.g. proning, timing of interventions, improved oxygenation, anti-inflammatories, anti-coagulants, antioxidants)
- Shielding vulnerable populations (e.g. vulnerable and older individuals, care homes
- Ecological control of disease (use of environmental and climatic factors and human behaviour to limit morbidity and mortality while maximising naturally-acquired herd immunity)
- Traditional vaccines, using attenuated (inactivated) virus (not considered feasible given intended number of vaccine doses required)
- Recombinant vaccines using genetically engineered protein fragments (plasmids) that encode for an antigen, combined with an adjuvant (e.g. an aluminium salt) that intensifies the immune response and consequent production of antibodies
- Other vaccination technologies
Many of these options have not been adequately explored. There is an increasing emphasis by governments that the only way out of lockdown is mass vaccination. The public is being told very little about how the vaccines are being developed (Figure 3), or what the implications of their fast-tracking might be on safety or effectiveness.

FIGURE 3. Pipeline of COVID-19 vaccine candidates by technology platform.
Source: Thanh Le T, et al. The COVID-19 vaccine development landscape. Nat Rev Drug Discov. 2020 Apr 9. doi: 10.1038/d41573-020-00073-5.
They are certainly not being told that the vaccines currently being developed are predominantly the product of genetic engineering. There is no public discussion over the risks associated with such fast-tracking vaccines.
When applied previously to GSK’s Pandemrix for the 2009 ‘swine flu’ pandemic, a slew of damages that governments have consistently tried to cover up were left in its wake.
The public is also not being told that nationwide vaccination under national immunisation programmes provides legal protection to the vaccine makers in the event of no-fault vaccine-injury. This contrasts with regular therapeutic drugs for which the pharmaceutical industry remains liable in the event of litigation based on conclusive evidence of undisclosed harms.
At ANH-Intl, in evaluating all the available evidence, we believe adamantly we could be afforded a much quicker and less damaging route through this current pandemic that wouldn’t involve causing such widespread collateral damage to societies and economies.
This would be a much more fluid system that would flex according to the needs of affected cities and towns. It would be country-specific and regional, not national or international, built around the circumstances, biology and ecology of the infection in a given locality.
It would include real-world trials in which immune enhancement protocols were prioritised, alongside improved antigen and antibody testing and shielding of vulnerable populations. It would include changes in acute care management that took into account the views of those at the cutting edge of clinical care who have demonstrated high levels of success with innovative strategies. This would include routine use of high dose intravenous vitamin C in patients with severe disease. It would include nutrition and lifestyle based prevention strategies that have been demonstrated to enhance immune function. People would also be asked to send as much time outdoors as possible; not only are respiratory infections 'caught' much less frequently outdoors, exposure to sunlight will increase circulating levels of vitamin D. What evidence did northern hemisphere governments rely on when telling their public to "stay indoors" after a long winter?
Bottom line, if governments were to listen diligently and with open minds to some of the key voices we’ve included in our video (below) along with the views of the many others with valid knowledge and experience who are also not being adequately heard – the strategies being employed would change dramatically from those currently being enacted. Lives would be saved and the future would be far brighter. We would have adapted to a new virus – something we’ve done successfully many times before in our evolutionary history. As importantly, the civil liberties that our ancestors have fought to ensure over centuries in the so-called free world would remain with us.
From infectious to social uprisings?
The road we’re on is undoubtedly a very dangerous one. The virus is likely the least of the dangers we currently face.
The arrest, bullying and albeit short detainment to a psychiatric ward of medical lawyer Beate Bahner in the southern German State of Baden-Württemberg serves as reminder of what can happen when government’s disregard the rule of law under the pretext of this pandemic. Ms Bahner’s supposed crime was organising a protest against the lockdown.
Civil unrest is building elsewhere, from Berlin to the USA, where protests have been witnessed in New York and Ohio, to name just two examples.

Last month, we urged our supporters that the key was to adapt, not fight. At that time we were only referring to dealing with the virus itself.
We now sense a different approach may be required to deal with the human, inter-governmental and governmental response to the virus. It seems more and more likely we will once again need to fight for the right to peacefully protest, to express ourselves freely and to care for our bodies in the manner we choose, even if that is by entirely natural means.
Check out our weekly update in the ANH-Intl Covid Zone
Go to ANH-Intl Covid Zone



Comments
your voice counts
17 April 2020 at 11:36 am
It may beggar belief as to why persistent liars are given attention, credibility and trust - over and over again.
The lie and the father of it, inherently frame us in conflict and division, distrust and self depleting and destructive patterns of thought and behaviour. But running or presented under pretexts of fear that invokes control.
Those WHO most deeply align in such identity - which may include us in our own triggered reaction - DO the thing they are saying they are defending against and have to be read backwards.
We are in the target frame as the 'viruses' just as we are in the target frame for carbon guilt.
Science is turned on its head by incepted idea given power and woven into the fabric of invested thought, policy and funding. THAT is the virus or malicious code that runs as a framework of currency of communication and exchange.
We are suffering from the massively disproportionate REACTIONS, born of terror by design under pretext of medical science. Why not unsub from Dr WHO, shut the Gates of hell and turn off the Fauci of lies? Nothing personal against the humans being such a role - but they are tooled by a hate agenda to put a human 'face' on inhuman agenda. I see no institutional Parent looking after our interests while civilisation such as we have known it, fails by design to operate fear and control in lockstep.
What is there to lose from our heart's decision to turn away from lies now and choosing to listen for truth now? Perhaps we seek to reform the 'system'? Rehabilitate global monopolists? Or a more reactive and vengeful or self vindictive set of mind?
Maximising the lockdown is flattening the consciousness.
Any string of pretexts to buy time the crash the global economy to a pre-planned command and control system - based on closed system (dead) physics at best, and serving tyrannous agenda and unchecked imagination at worst.
All of this top-down manipulation operates attack on Reason, as the true willing alignment of our Heart's desire as our Consciousness and Cultural expression. Deceits only run because we accord them meaning and allow our sympathies to be enlisted, to be baited and framed in our own invested narrative identity.
Yes in practical terms we still have to discern and navigate the world of what is due unto Caesar and what is due unto God - as the Creative Source and Nature of our being - including the freedom to refuse to accept love. In other words these are not at war as polarised good and evil, excepting we frame ourselves in the narrative of the attempt to eradicate freedom as if such a mind can be anything BUT self-isolated dissociation.
Many are currently choosing to reinforce a bubble of fear-driven guilting, shaming and denying hate as a narrative identity of collective virtue signalling. Perhaps mostly in a very short term drive to mitigate an intolerably disturbing fear. This is potentially very volatile and calls for discernment and compassion which embraces what is actually here - in the Field of relation - in willingness to serve and align in the movement of a wholeness of being.
Accepting our primary responsibility for Consciousness enables releasing what never was our responsibility. How much if any of what fear and guilt demands and coerces (by our own thought or others) is in fact within our capacity to perform, live up to or control?
Trying to be (or live up to) what we are not, costs the awareness, appreciation and sharing in who we truly are. This is also at times very messy, unsettling and thus a call for renewing our mind from a willingness to listen, to tune in to the signal beneath the noise rather than tune into invested narrative reinforcements by blocking or killing the Messenger.
But at this time both are in our minds and being exemplified in our world.
Choices are made by our alignment of attention and intention, often as an unconscious default.
17 April 2020 at 6:39 pm
Brian - we love to hear your inner wisdom, as I'm sure do our readers. Thank you. Kind regards, Rob
17 April 2020 at 4:05 pm
I fully agree with Knut Wiskowski, who uses logic and common sense, and his recommendations are clearly the ones that should have been adopted and would have avoided this completely unnecessary lockdown and the removal of our freedoms. I strongly disagree with the Covid smorgasboard with its nonsensical proposals, which would only exacerbate the mess that has been created.
In any case, it is eminently conceivable that the suspicions eloquently presented by Brian Steere go to the heart of the matter and represent a foretaste of what is to come.
18 April 2020 at 6:38 pm
The daily updates during which journalists have been asking questions have been disappointing as the Government's Scientific Advisory Group for Emergencies (SAGE) is not being transparent. It has become so obvious that I think those who didn't realise what the government is capable of when it comes to not providing reliable and transparent health information may well start having their suspicions that they are being let down. That would be a good thing!
24 April 2020 at 1:04 pm
I think what is really important here, in addition to discussing the ins and outs as in this brilliant and informative article above, is what we citizens can strategically do. A) I suggest we all contact the local hospital in our region, asking them to use IV Vitamin C. Invoke the appropriate laws, and send them a package regarding the science involved. Dear ANH, can you please provide us with a URL link containing legal and scientific information for hospitals that we can all send along? Thank you. B) I think the problem with implementing the brilliant strategies offered by the ANH in this article above, including such commonsense measures as treating the virus uniquely to each country and its health climate and its environment (imagine that??), is that people just commonly believe that vaccines are the sole solution. Education of the governments, and the masses, would seem to be key. I ask for communal brainstorming, and suggest that the ANH hire several political strategists, to help to this end, and fast too. We are on the brink of world dictatorship, which is not a funny prospect at all, and have a narrow corridor of time. But corridors have exits, beyond which windows of light exist. I think such education must stress the science in natural medicine as options in addition to vaccines, and specifically how they work. C) Political strategists might advise how to cut through the media blackout. I have a few ideas myself, but am concerned if posted, they may be intercepted. This is information that needs to be relayed orally, to the ANH, by experts. Please consult and then advise us thereafter, what to do. Meanwhile, We the People can quietly start appealing to underground sources for public education, which is desperately needed. Facebook is NOT the only way to go, and is censoring (Sue 'em! Call them out on the law and on blogs, and urge boycotting!) D) During times like this, the public does not think logically. Instead, they think emotionally. The higher ups know that, and seem to have engineered the climate exactly to that end. Political strategists should be asked how to work effectively within this highly emotionally charged climate. Readers, please weigh in with your responses. Thank you all, and thank you ANH for your brilliant work. We really appreciate you deeply. You are important.
24 April 2020 at 1:25 pm
I am asking that we readers please contact attorneys who have big power and big success records. Businesses, large and small, that have lost out due to the economic shutdown, might want to get on board, class action, please write to them too. Please send URL links to underscore:
https://www.youtube.com/watch?v=A71lfXrQlxU
https://www.youtube.com/watch?v=eEup9pErtmM
Someone has got to Shut the Gates of Hell. Not just shut him up (how does one man get to run the world by the nose, practicing global epidemiology and world-wide medicine without a license in either one?) but to take him out of power. https://articles.mercola.com/sites/articles/archive/2020/04/21/bill-gates-political-power.aspx Bill Gates said on film, that (Specifying) to be very clear, he does not want the masses to heal as a result of this shutdown. Instead, he wants the 1% shielded by the virus, and he called it "economic pain" for the rest of us, which he thinks will effectively shield the 1% from the contagion. He spoke years ago about sheltering in place, the meeting in NYC with Bill and Melinda Gates drilling for an outbreak of a virus known to cause severe respiratory distress preceded the announcement of the outbreak, and here we just sit quietly, passively, Playing Victim. We can only be victims if we allow ourselves to be. How can billions the world over, have less power than one single man, no matter how interconnected, wealthy and powerful he is? It's time for the power of the many to peacefully, legally and effectively, triumph over the Single. Given the impact to the economy and ourselves, and all this man has said on film, why can't we win?
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences