

Content Sections
Note: You will see an advertising banner beneath our videos that play off the Brighteon platform (when they are not maximised). This advertising helps support the Brighteon platform that doesn't charge subscribers for their content, is committed to free speech, yet is also respectful of copyright-related law. We'd like to clarify that no advertising revenue from Brighteon is received by the Alliance for Natural Health Intl.
Video transcript
Hello – my name’s Rob Verkerk – I’m the founder, executive and scientific director at the Alliance for Natural Health International – and I’m here for another ANH coronacast – this one focusing on the hot topic of whether and how schools might or should reopen.
I speak to you not only as a sustainability scientist – but also as a parent. My oldest is a surgeon in the UK’s NHS and has had to deal first hand with some of the complications from severe disease and ventilator support. My youngest two are still at home, doing their best to do distance learning, in many ways having to learn ways of learning that we’d previously thought were challenging even for first year undergraduates. Now we expect it of primary school kids. Yes, so I declare my interest too as a concerned parent.
-
Find related articles, information and videos in our Covid Zone
What this video is about
In this video, we’re going to be looking at
- the state of the science,
- what children’s and teachers’ susceptibilities to covid disease might be
- if kids really are the super spreaders the media makes them out to be
- if teachers and schools are justified in their claims that schools will become death camps if they’re re-opened
- if school re-openings could contribute to another wave of infection and finally
- what kinds of strategies – based on the existing scientific evidence – should be put in place to protect children, teachers, other staff and the community at large when schools are re-opened.
Science dive
Ok – so let’s dive into the key science. First thing to note is that it isn’t going to be the deepest dive – that’s because the science is somewhat thin on the ground. This of course breeds uncertainty and it’s also interesting given this situation that some elements of this limited science have been picked up by the media and been badly misrepresented. That’s all well and good if the idea is to instil fear in the public – which it seems is exactly what the UK SAGE group – that’s the scientific advisory group for emergencies that advises the UK government has been doing. Here’s a leaked copy of the minutes from one of the key advisory groups – the so called Independent Scientific Pandemic Influenza Group on Behaviours or SPI-B – that itself feeds into SAGE from late March. It shows clearly a calculated approach to combine persuasion, coercion and other tricks widely used by unscrupulous ad agencies and totalitarian governments to instil fear in the public to make us, the public, malleable and responsive to government policy – however weak the science it was based on.
The media have been deliberately engaged as propaganda agents for this purpose – so no wonder censorship of any dissenting voices has been running rampant.
This might be all very well and good when you’re trying to push people into lockdown – not so good when you’re through the main wave of infection as we now are and trying get kids back to school and people back to work.
Now the UK government especially faces a very reticent response from many teachers, schools and governing boards – as has become more and more commonplace the government position is often bumbling, contradictory and undecided.
BBC News: Schools safe to reopen, Michael Gove insists
The Mirror: Ministers have 'no idea' if reopening schools will cause second coronavirus peak
The Independent: 'I don't know': Plans to reopen English schools next month up in the air after minister admits growing revolt
With a trail of mistakes behind it – it probably wants to limit further mistakes. One way through this is to do what the Swedes, Danes, Fins and many others have done – open schools or in some cases have never closed them. Use all of the science to make the most informed choices that minimises the net impacts on society.
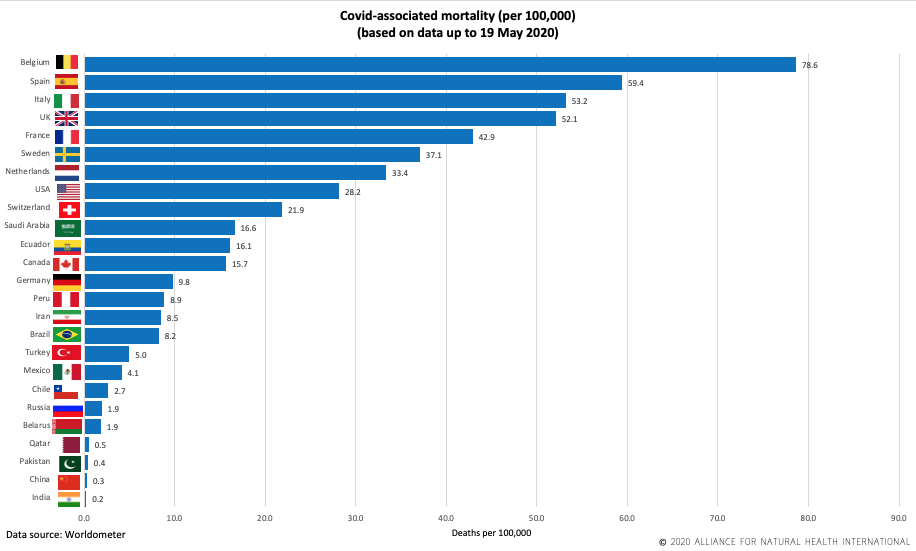
And it’s interesting if you look at the latest figures on mortality rates per 100,000 population across the 25 countries in the world with the highest incidence of case rates as we show here there’s no evidence that those who left schools open had the highest incidences of serious disease. In fact, quite to the contrary. All four countries that hit mortality rates of over 50 per 100,000 – the top 4 on the chart – all closed their schools.
Expert view
So let’s look at what paediatric or child health doctors and researchers have to say. Here we find it hard to disagree with the views of Drs Alisdair Munro and Saul Faust who piggyback between the University Hospital Southampton NHS Foundation Trust and the University of Southampton. They have no competing interests – their funding coming from the UK’s central research funds through the National Institute for Health Research. No hint of any Gates Foundation money there then.
They make it very clear that it’s time for the kids to get back to school. Here’s a few extracts from their article published on 5th of May.
If, as for influenza, children are the primary drivers of household SARS- CoV-2 transmission, then silent spread from children who did not alert anyone to their infection could be a serious driver of community transmission. On this presumption but without evidence, school closures were implemented almost ubiquitously around the world to try and halt the potential spread of disease despite early modelling that suggested this would have less impact than most other non- pharmacological interventions.
Munro and Faust make the point that the original idea of closing schools came about because it was assumed – which turned out to be a wrong assumption - that kids were super spreaders, just as they can be with other respiratory viruses – especially flu. We now know that’s just not the case.
They then go on to summarise the available evidence concluding that kids have very much less serious disease than adults representing less than 2% and sometimes less than 1% of those infected. Most are either asymptomatic or suffer mild symptoms and nearly all make a full recovery. In actual fact other respiratory viruses like flu and certainly RSV – respiratory syncytial virus – hit kids a lot harder than covid – and schools have never been closed for these viruses.
Evidence is therefore emerging that children could be significantly less likely to become infected than adults. On the other hand, children could have a more transient upper respiratory infection with minimal viral shedding, or the less likely scenario of showing minimal symptoms despite significant viral shedding. A further key question is the ability of infected chil-dren to spread SARS- CoV-2. A collection of international family clusters found that children were not likely to be the index case in households, only being responsible for around 10% of clusters. Data from Guangzhou have supported this, finding an even lower rate of children as index cases in households at 5%.
Another key point that emerges when you look at the balance of evidence is that children are much less likely to spread infection – based on studies of familial clusters from China and Italy.
Everyone’s now very familiar with the fact that there are a particular cluster of symptoms including hypertension, type 2 diabetes, obesity and a history of lung disease that make adults very vulnerable. There’s no similar clear picture with children. That even goes for kids who are clearly immune compromised – or immunosuppressed even by drugs. It suggests there’s something else going on with children – and that might be down to their lively innate immune systems that make it harder for the virus to get a foothold and it then means they don’t suffer all the issues of a delayed over response or cytokine storm from the adaptive immune system that’s linked to most of the cases of severe disease in adults.
Understandably – that means that a lot of paediatric doctors are actually not so much concerned about the virus – they’re more concerned about the disadvantage that will face so-called vulnerable children if they’re not allowed to return to school as against healthy kids who can.
Many paediatric specialists are concerned that a blanket assumption that immune- suppressed children of any kind are all at increased risk will cause consider-able long- term educational and social harm to these children. At the current time, children do not appear to be super spreaders.
Munro and Faust don’t beat around the bush. They make a direct call on governments worldwide – based on the available science – to allow ALL CHILDREN back to school, regardless of comorbidities.
Governments worldwide should allow all children back to school regardless of comorbidities. Detailed surveillance will be needed to confirm the safety of this approach, despite recent analysis demonstrating the ineffectiveness of school closures in the recent past. The media highlight of a possible rare new Kawasaki-like vasculitis that may or may not be due to SARS- CoV2 does not change the fact that severe COVID-19 is as rare as many other serious infection syndromes in children that do not cause schools to be closed.
Well we agree with them.
The reality is there’s been a misguided reaction from either misrepresented science or early studies that have now been disproven that continues to bolster a view among teachers, their unions and governing boards that it’s way too early and way too dangerous to reopen schools.
Misrepresented German viral load study
One piece of influential research – a German study – misplaced as its conclusions are – is that children can have the same viral load as adults. The conclusions make it abundantly clear that the viral loads of the very young – the under 10s don’t differ significantly from adults.
The problem is that the data in the paper don’t reflect the authors’ conclusions. There are some real issues with this study – which hasn’t undergone peer review, like so much many of the studies being published in journals during this crisis. What the authors are looking at are statistical artefacts in their analysis where the variance appears to cancel out differences. But there’s a problem with their methodology.
If you look at the raw data you’ll see huge differences in viral load that fit much better with the balance of evidence – not that the media has taken much notice. After all, why would you want to quell the fear when you’ve been asked to work with governments to maintain it.
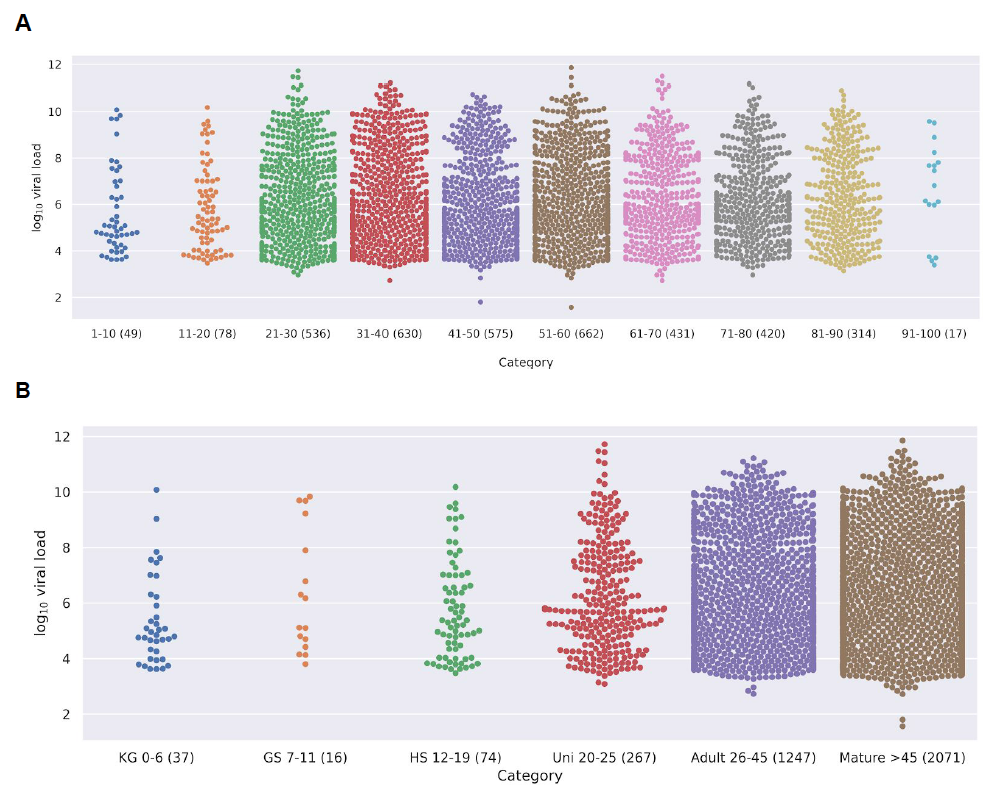
You can see this clearly in Graph A for different age groups, each with 10 year intervals. You’ll see much lower viral loads in the 1 to 10s and 10 to 20s compared with the adults groups. You also see it by schooling or social group in Graph B – the kindergarten kids on the left side, as well as grade school and even high schools kids show much lower viral loads than the adults over 26 on the right side.Iin the final figures in the paper that show from top left, younger adults from 26 to 45 years old, through to grade school kids aged 7 to 11, high school kids aged 12-19, kindergarten kids aged 0 to 6, mature – the over 45s and then university students from 20 to 25. Check out the y-axis scales and note the huge differences in viral loads in the young adults, top left, and mature over 45s, bottom left – compared with everything else.
Based on this paper that was used by the media to push the idea that kids have the same viral load – it would be safe to say theirs is around one-third of a typical adult. Not only that the current data – based on the other studies showing they are rarely the index cases that initiate clusters of infection – shows they are much less likely to transmit the virus.
What about Kawasaki-like syndrome?
What about the Kawasaki-like hyper-inflammatory syndrome that’s now hit the media and got the schools so agitated about going back?
The first thing to say is the science is not fully resolved around this – it’s a newly identified syndrome and it was in fact a UK study that created a national alert.
From the emerging evidence it appears that a very small number of children are at risk of a Kawasaki-like hyperinflammatory response syndrome that appears associated with covid infection. Common symptoms are abdominal pain, diarrhoea, gastrointestinal symptoms and a persistent fever. Since the UK raised the alarm bell it’s also been noted in China, the US and Italy.
-
We're funded only by donations. Any amount is welcomed to help us continue our work
In very rare cases it can lead to multi-system organ failure – but even the WHO considers the rare condition to be treatable with parenteral immunoglobulin and steroids.
Interestingly - a study on Kawasaki disease itself from 2015 showed that 99% had low levels – less than 75 mmol/L, or 30 ng/mL in US money, of circulating hydroxy vitamin D compared with 79% in controls. More than that, those who had very severe symptoms including developing coronary artery abnormalities had severely low levels between 12 and 38 mmol/L – that’s 5 and 15 ng/mL in US units.
Sadly the government advice on vitamin D consumption also flies in the face of the scientific evidence. They’re saying you need just 10 micrograms per day – that’s just 400 international units. But what we really know about vitamin D is that individual requirements are linked to differences in metabolism – remember vitamin D – in its active forms 1,25 dihydroxy vitamin D, is a hormone and precursor to all our steroid pathways as well as being an anti-inflammatory agent and immune modulating factor. Over 3 years of evidence shows us that intakes don’t correlate well with circulating levels of the active vitamin. Measuring your circulating levels of 25-hydoxyvitamin D and metabolites is a much better way of doing this and for kids over 1 you need to be in the ballpark of 50 micrograms or 2000 international units daily to make sure you hit the sweet spot - 100-150 nmol/L or 40-60 ng/ml in US units - in terms of your circulating levels – and that’s even if your requirement is higher for genetic or physiological reasons – and assuming there’s no significant sun exposure. You can double this or more for adults – based on body volume.
Do You Know Your Vitamin D Level?
Find out with our home test kit.
Research has demonstrated many health benefits of higher vitamin D levels. What do scientists say is the target amount? 48 world-wide vitamin D researchers agree it is 40-60 ng/ml (100-150 nmol/L). Determine your level today
It’s then particularly interesting that the kids suffering the most serious Kawasaki shock-like symptoms are those who suffer the greatest physical challenges and require the most technological support and probably spend the least time outdoors – and may not consume a lot of the foods like oily fish, egg yolks or mushrooms that are natural but limited sources of oral vitamin D.
Leading UK paediatricians provide guidance
So what does the UK’s most important medical college for paediatricians – the Royal College of Paediatrics and Child Health – (RCPCH) probably the very group of medics with the greatest insights on children’s health – say about all of this.
The RCPCH has put together a comprehensive summary document that should really be the key guidance documents that schools refer to. In our view it reflects the balance of evidence around covid impacts on childrens’ health and risks to others really well.
The 101 from this document looks something like this:
- Very low incidence of Covid-19
- Critical illness and death very rare
- When present, mild symptoms or asymptomatic
- Common symptoms cough and fever
- Acquire infection less easily than adults
- Low transmission potential
- Viral shedding for 6-22 days (median 12 days)
- Vulnerabilities unclear
The incidence of Covid-19 symptoms is very low – less than 2% of all cases, and even less among the youngest groups. Kids very rarely get seriously ill or and it’s extremely unusual for them to die – and generally only when there are other, serious complications. This risk is actually quite a lot less than with some other respiratory viruses such as RSV that’s never caused school closures. When kids ecome infected, based on testing – most of the time they either get mild symptoms – mainly coughs and fever – or they’re entirely free of symptoms. They not only get infected less than adults – just as importantly – they also pass on infection less easily to adults, as shown by how uncommonly they have been found to be index cases in clusters identified through test, track and tracing schemes. Viral shedding duration is also important if quarantines are going to be considered. The range varies considerably between 6 to 22 days with average or median of 12 days.
Finally the picture on children’s vulnerabilities is definitely unclear – and contrasts greatly with what we know about adults and the well-known comorbidities that greatly increase their susceptibility. The very few kids who have been most severely affected have been those with very complex conditions, including disabilities and genetic abnormalities that require them to be dependent on long-term technological support.
What’s more of a surprise is the evidence shows kids who are even immunosuppressed – either as a result of disease or immunosuppressant drugs – are not more susceptible. But the RCPCH still concludes the risks even to the most vulnerable groups isn’t any greater than any other respiratory viruses.
So how does all this science inform decisions to move forward – to proceed with opening schools – or hold off until later?
We absolutely concur with the findings of the Royal Society of Paediatrics and Child Health. They point to an evidence summary that’s very useful on a really great and important website run by a bunch of Australian and UK paediatricians called Don’t Forget the Bubbles. The Covid Resources is especially useful when it comes to kids…
In it you’ll find a page that summarises all the relevant evidence relating to kids and Covid-19. There’s nearly 200 papers referenced there – and these are the people saying it’s time for kids to go back to school. So please listen, dear governments, teachers’ unions, school governing boards and parents.
Or if you don’t choose to listen – please don’t profess to be guided by the science.
Other countries?
In fact a quick squiz at what’s being going on in Sweden is very informative.
No school closures ever occurred for primary and junior school kids and there is no evidence at all for any increase in community infections linked to children based on test, track and tracing. That’s very useful evidence that fits well with what we know about how the virus behaves around children.
It’s a bit too early to tell from the data from Germany and of course the 70 cases in France have hit the news big time and got everyone panicking again
It’s hit the same old, well-worn fear button in the minds of many – teachers, governors, unions and parents alike.
But when you drill down into the data it doesn’t wash with the overall trends.
Here we see very clearly that when you look at the 22 EU countries that have been reopening schools there has been no spike. None.
In fact if you go back to looking at EuroMOMO data – you’ll see very clear evidence that excess mortalities in children have never spiked – and in fact in of all the 24 European EuroMomo countries including the UK, there’s been lower incidences of death – note the dark blue lines for 2020 in the 0 to 4 years and 5 to 14 year old categories – as compared with 2018 and 2019, since the covid crisis began.
I want to just finish off by offering some views on how we think – again informed by the science – including an assessment of risks and benefits – kids can be brought to schools, safely.
For a bit of context on this point – and you may have noticed we’re great fans of context at ANH – the World Economic Forum estimated a few days ago that there are around 1.5 billion kids facing some kind of restriction to their learning at school because of Covid-19 and 60% of these live in countries with partial or full lockdowns.
It’s such a big issue – because we’re playing here with the generations who will in the not too distant future be running the show here on planet Earth.
ANH proposed school reopening strategy
Cutting to the chase, here’s our summary position on some of the main areas we think should be on the top of any list of strategies for school re-opening – and that’s based on our detailed assessment of the current scientific evidence:
- Staged school reopening – youngest ages, smaller schools first
- Infra-red temperature recording at least twice a day at school (e.g. start and finish)
- Regular, supervised handwashing with regular soap
- Staff trained to identify and report symptoms
- Test, track and tracing system must be in place
- Quarantining following identified cases and exposures
- Antibody testing offered to staff who have previously experienced Covid-like symptoms
- No distancing in classes, but additional time spent outdoors (normal activities)
- Staff considered vulnerable should avoid returning to schools
- Mask use by staff optional, although visors that don’t interfere with non-verbal communication are preferable
- Advice given to parents on maintaining or improving immune resilience
It makes sense to stage the opening of schools starting with the youngest kids who have least risk from the coronavirus – the kindergartens and primary schools – first, as well as smaller schools. This means that in the event of an infection cluster developing, it’s going to be smaller than in a large school. It’s a bit like putting your child who you’ve just taught into a new swimming pool for the first time. You’d choose the shallow end – rather than forcing them to jump into the deep end. As important as any risks from the virus, is building confidence among the staff, parents and wider community – and that’s also a bit like learning to swim again.
Then – let’s not get hung up about temperature measurement. With today’s non-invasive infra-red thermometers – there’s no contact, there’s no associated surveillance. It just makes everyone feel safer if we know that all the kids coming into the school gate don’t have one of the main symptoms of infection in kids – fever. If you do find fever – you kick off the test, track and trace system that should be run by local councils. Temperature recordings could also be done at the end of the day.
Regular handwashing has obviously got to be on the agenda. But that doesn’t mean over doing it or using toxic antibacterial agents that damage kids’ sensitive skins or give them rashes and other dermatological problems.
You need the staff to know how to spot symptoms and report them – and you also need a fully operational test, track and trace system – as used so effectively in countries like Taiwan, South Korea and closer to home in Denmark and Finland. In the UK this has been a long time coming and we’re still not there - but we’re told it’s imminent.
If you’re going to have a track and trace system – you also need to have a quarantine system. In our view quarantining the small number of people who might initiate further transmission in the community is way preferable to locking down the whole of society or disadvantaging those kids who don’t have the space or environment to work effectively from home.
Back to testing – with all this talk about testing – and the huge numbers of tests that are being conducted around the world – let’s remember the vast majority of these are antigen tests that tell you only if you have the disease, not if you’ve had the disease. That’s all very well and good if you’re looking at the early stages of an epidemic or pandemic or if you’re using it to track and trace new cases.

But now – as we’re well along the infection curve and down the other side – we really need to see antibody testing ramping up – and not just being made available privately for those with the money to part with a couple of hundred or more pounds or dollars.
Knowing you’ve had the infection in the past – or not as the case may be – is really important to getting people back to work – as well as building confidence. It’s maybe not all governments’ highest priority if they’re hedging their bets on letting us all free when a vaccine finally comes on tap – but for the rest of us it’s a really important way of determining if you’ve got immunity. In our view it should be available to all staff in schools – and the use of antibody tests could be a vital tool in rebuilding confidence and dispelling fear in the community – fear that was deliberately engendered by those responsible for public health strategy.
Now – we’re going into probably the most controversial area. We’re advocating for no social distancing in classes. Just normal school. And we’re not the only ones
We’re thrilled to see the Us for Them campaign building in the UK that’s saying social distancing in schools and nurseries is not OK. Let’s see that #NotOk hashtag come alive – it will have to compete with the #schoolsreopen that’s being pushed very hard by those who have an irrational fear of the virus generated by the government and pro-vaccine propaganda machines.
Talk to primary school teachers and educators – talk to behavioural psychologists. Talk to therapists who deal with children or adults who’ve not had the chance of close bonding with those around them. We have.
The only way to look at this is by weighing up risks and benefits that affect all those affected, from their different backgrounds, ethnicities and cultures, taking into account the even greater social and educational inequities that impact the most socially disadvantaged.
Then you have to accept – based on the science – that the risks to kids themselves are comparable or even less than other respiratory viruses for which we haven’t enforced social distancing or school closures. If you’re going to implement social distancing and put pupils into bubbles, and force them to sit 2 metres apart in classrooms and avoid any form of contact – there has to be a very good scientific reason to do this. And those reasons simply don’t exist.
You’ve got to also consider the impacts of social distancing and related measures to the learning and developmental process. Plus there are other measures to guard against any shift of infection back into the community – which the science is telling us is highly unlikely in any event – like test, track and trace systems. So why do we need to so severely disrupt the learning environment?
OK, then there’s the potential risk to adult staff – but the plus side is the science here shows we know a lot about the vulnerabilities among adults. So if we have shielding for vulnerable staff members in place – with those staff who’re considered vulnerable not returning to school while there’s virus in the community or at least avoiding any proximity with others who might be infected – the risk to adults can quite easily be mitigated without massive disruption to the kids themselves.
While we’re talking adults – I’ll add that that we’re not great fans of masks for the general population given the variable science on their benefits outside a critical care environment. That applies even to N95 respirators or surgical masks in schools. You’ve got the problems with resourcing, of disposal and the risks of contamination. You increase the risks for users who in this case are more vulnerable to covid than those they seek to protect – the kids. The fact is the actual risk profile in schools is low because kids appear to not be good spreaders. And then you’ve got the fact masks have a big impact on the ability of young children especially to read non-verbal, facial communication.
For anyone interested in this I suggest you have a read of Dani Hall’s great blog called the Smile Behind the Mask on Don’t Forget the Bubbles.
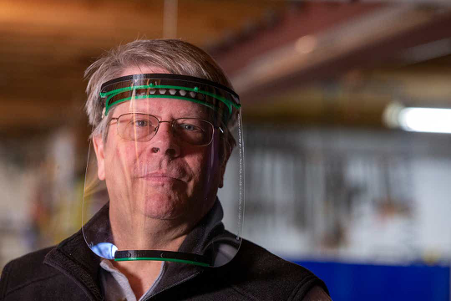
There’s a lot that can be done for those who choose to use some sort of protection – and yes, we think it should be optional not compulsory. Visors make a whole lot more sense than masks especially around young children if some kind of transmission protection is considered necessary given the most common form of transmission involves droplets from spluttering as people speak with each other.
 bubble
bubble
Source: Smile Behind the Mask
So check out how a young kid might respond to someone with a visor as compared with someone with a mask.
Source: Northjersey.com


And I just want to finish up on one more point – one that’s been roundly ignored by governments. What we do to help people – both kids and school staff – to optimise their immune resilience. It’s far too big an issue to cover in this video so let’s look at this as more a placeholder given there’s a lot on our website about this and you’ll find links to this below.
But helping kids to reduce any excess weight, to be very active, spending lots of time outdoors getting themselves in the dirt so they can develop their all-important external and internal microbiomes, eating balanced, varied healthy nutrient-dense diets along the lines of our Food4Health guide, taking additional vitamin D if they’re not in the sun, keeping vitamin C, zinc and other nutrients topped up, all of it is crucial.
In the Philippines they even dish out vitamin C to the kids at school. And let’s not ignore the fact that with it’s nearly 110 million strong population it’s only reported around 850 deaths from Covid-19.
Another point is that we know that kids come into this world with a powerful innate immune system that’s the first response side of our immune system that’s the body’s first attempt to deal with any invading pathogen – suggests keeping your and children’s innate immune systems primed is pretty important.
Concluding remarks
So that’s our take, based on all of the existing, albeit sometimes limited or incomplete science – on why and how we think schools should reopen.
You’ll find a lot more information on our website – all of the content including articles, videos and weekly updates on the science and media around covid – curated in one place at covidzone.org.
Our main website is anhinternational.org
Thanks for watching – and if you like what you’ve heard or seen, please subscribe to our censored Youtube and uncensored BitChute channels – and greatly look forward to seeing you next time.
>>>Return to ANH's Covid Zone
>>>Return to the ANH homepage


Comments
your voice counts
22 May 2020 at 9:00 am
Well done Rob, I've not read every word but more than enough to see you are talking sense. It occured to me that the issue we face is one of giving too much autonomy to head teachers. The UK was slow to shut down because it was hard to enforce it in a free democratic society. We now face the other end of the problem. We should have had a much clearer statement about when the lockdown was going to end. The scaremongers are now ruling the roost with emotion rather than science. Headteachers have no responsibility for the downsides involved in maintaining lockdown - they are not taking a view that balances the realities government has to include. Looking at the natural distribution curve we can see the threat of Covid-19 is now lower than many other threats. That, surely, should have been flagged up as the point lockdown was no longer going to be worthwhile. With children proving to be far less likely to suffer or spread the disease there are going to be far more suffering from other problems - such as sport injuries or the everyday danger of crossing a road. We don't go far if we don't cross a road at some point!
22 May 2020 at 12:42 pm
Checkout Naomi Klein in 'Screen New Deal' - Silicon Valley are poised to facilitate distance learning ! Could this add to the strategy behind the fear ? Klein is presented as a univesity research professional and appears to be a system / state emissary. Her discussions finish with a look at technological progress in China where, unfettered by 'rights and freedom' great advances have been made in surveillance using AI - Artificial Intelligence. The tone of the message is such as to inject enthusiasm - could this be the new space race ? !
22 May 2020 at 8:42 pm
Brilliant article. My friend’s daughter is not going to send her child back to school ,not because of the virus but the fear that the social distancing practises are going to have on her. Social distancing needs to be stopped especially in children.
23 May 2020 at 8:15 pm
I wholeheartedly agree with you Avril. Applying these unsubstantiated rules to children would be bound to cause untold social damage and mental health issues in the future. If I were a parent of school age children, I should withdraw them from school, like your friend, for fear of the damage that the distancing (I won't call it 'social') would have on them. The whole thing seems like a totally irrational, hysterical reaction, with no scientific justification. Unfortunately though, parents in our area are still mostly afraid of the children catching and transmitting the virus and this would be the main reason for not sending them to school. I keep sharing information from ANH and hoping that eventually people will have more courage to think for themselves and question the official agenda. Thank you Rob and the team for all the assiduous research and brilliant presentations. They are so important.
22 May 2020 at 9:20 pm
Brilliant. Thank you Robert.
24 May 2020 at 11:13 am
Hi Rob. Excellent article - provides the scientific backing to support something that should be at the top of our agenda: getting schools reopen and not trashing the education of a generation. The continual presentation of headline data on COVID without the importance nuances you highlight - around age / infection rates etc - isn't helping. You are absolutely right to highlight that the core debate for schools should be to protect those school workers who are in vulnerable groups (over 60 / underlying medical conditions etc) and not mix this effort with extra steps which are causing so much anxiety (like the social distancing in classes which are patently going to be hugely stressful to manage and, one would hazard to suggest, be totally unworkable for young children).
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences