

Content Sections
By Rob Verkerk PhD, founder, executive and scientific director, ANH-Intl
"I suppose the process of acceptance will pass through the usual four stages: 1. This is worthless nonsense, 2. This is an interesting, but perverse, point of view, 3. This is true, but quite unimportant, 4. I always said so."– J. B. S. Haldane, British geneticist and evolutionary biologist (1992-1964)
It’s been well over 2 years since SARS-CoV-2 was first identified in people in Wuhan, China in late-December 2019. But increasing evidence suggests the virus was circulating at least 2 months before this date.
But you can go back further in history if you look. That’s exactly what Albert Bosch’s team from the University of Barcelona did after they found samples of sewerage wastewater in Barcelona that tested positive in December 2019. They went on to analyse frozen historic samples and found samples that tested positive from as early as March 2019, over 3 years ago. Bosch’s study was reported by Reuters so it can hardly be dismissed as conspiracy theory.
Now, take in the fact that many countries around the world have experienced four waves of SARS-CoV-2 over the last 2 or 3 years. That’s a lot of virus that’s replicated in a lot of people – and a large proportion of this genetic material ends up in sewerage and wastewater given viral particles are readily shed in faeces, urine and saliva.
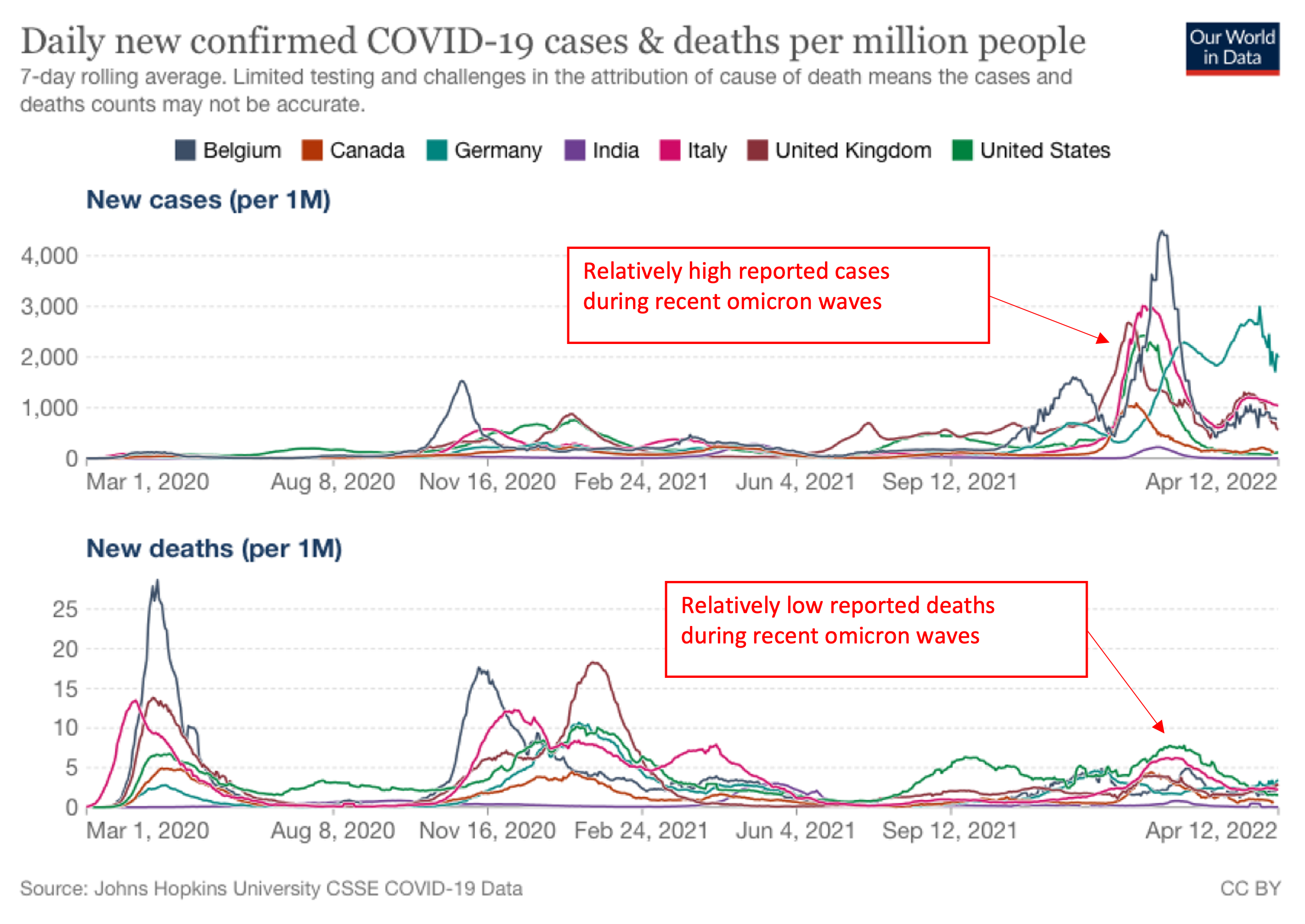
Figure 1. Comparison of new cases and deaths (per million population) in selected countries over the pandemic timeline. Source: Our World in Data (13 April 2022)
That’s not all. Some 65% of the world’s population has had at least one genetic vaccine that produces spike protein in the body. That’s not viable virus, but it’s spike protein, that is likely the main component of the virus responsible for disease in humans. That’s if you’re prepared to believe a major study by one of the foremost research institutes in the field, the Salk Institute, at least. And not believe the so-called ‘fact checker’ (aka narrative checker) journalists (e.g. here and here).
Enter WBE: wastewater-based epidemiology
The field of wastewater-based epidemiology is now a burgeoning field. Now that genetic sequencing methods like PCR have been rolled out everywhere, you can test sewerage and other wastewater to get an early indication if an outbreak is about to happen.
You might argue you’d see a coming outbreak quicker if you tested people rather than sewer water – but the reality is only a small proportion of people are testing regularly, especially if they feel healthy. So lifting manholes, collecting and analysing waste water samples has been something that’s being done for ongoing surveillance, including on university campuses.
In September 2020, the US Centers of Disease Control and Prevention (CDC) launched its National Wastewater Surveillance System to help provide an early warning of SARS-CoV-2 spread in communities. It’s a plausible way of doing surveillance given it's selection agnostic and it might give you a few days warning if infection levels in the community are increasing. But what are you to do with the information? Lockdown those who’re most susceptible, give them preventative therapeutics or jabs, or just elevate their level of fear?
Remdesivir – the best antiviral: really?
Speaking of therapeutics, the emphasis on remdesivir by health agencies around the world shows you just how far off track we’ve (sorry, they’ve) got. This is an antiviral developed by Gilead Sciences initially for hepatitis C, that failed, that then had an outing for Ebola, that failed, that was then wheeled out for covid-19. Judging by its inclusion as a key therapeutic agent on the approved drug lists of most health agencies, you’d think the trials had been successful. Far from it. The one published in the New England Journal of Medicine that resulted in its approval in the US, UK and EU didn’t even find a statistically significant effect. The latest large-scale European DisCoVeRy trial found: “Remdesivir use for the treatment of hospitalised patients with COVID-19 was not associated with clinical improvement at day 15.”
I’m not saying the NIH and Gilead have engineered remdesivir’s position as an authorised drug for treatment of covid-19. But I am implying it. What’s even more outrageous is that the FDA has approved its use under emergency use authorisation for babies of 3.5kg body weight or more. Here’s Gilead’s boast about it. The decision is a scientific and regulatory travesty given the lack of data and lack of understanding of long-term consequences. Made even more blinding by either the absence of any recommendation for vitamins D, C or zinc, all with much better evidence. Or, as the UK has done with its NICE guideline, suggested that 10 micrograms (400 IU) a day of vitamin D is the only nutrient that is helpful against covid-19. That’s blatantly rubbish and this trivial amount of vitamin D based on bone health not infection data is desperately low and not in any way science-based.
>>> Find out more about ANH Intl’s Test & Take Vitamin D campaign.
Losing sight of the real problems and solutions
Frankly, given the present low risk of severe disease posed by the virus (Figure 1), it’s our view that we should only be responding to symptoms of this or any other respiratory or other infectious disease in at-risk populations. Health care systems need to get back to doing proper healthcare, in all its guises, not chasing after one pathogen that appears ever more likely to be a product of gain-of-function research (see here and here).
If disease is asymptomatic or mild, it means that the virulence in a given population is either low (and should be, relatively speaking, of low concern) or that group’s immune system is doing a great job stopping the consequences of infection becoming more serious. That’s a good enough reason to try to stay as healthy as possible – to highlight one of the most spectacular misses of recent public health policy in the vast majority of countries over these last two years.
Back into the sewers
Let’s get back to the place a large element of shed virus and spike protein ends up: the sewers.
>>> Read review on SARS-CoV-2 in wastewater
Try digging out some reliable data on spike protein in drinking water and you’ll struggle. I did at least, even with four decades as a researcher under my belt. Does that mean no one’s interested, the data’s hidden from public sight, it’s so obviously not going to be a problem there’s no point researching it, or ‘they’ just don’t want you to know.
One review suggests given that some water treatments reduce or remove some pathogens, the risk of infection by SARS-CoV-2 in drinking water is low “if proper precautions are taken” during water treatment.
That view is based on there not being a significant transmission risk from whole, viable virus particles. It doesn’t tell you anything about spike protein that’s about one-tenth the length of the typical diameter of a SARS-CoV-2 particle, which, you’ll remember (if we ignore the Salk Institute findings) isn’t meant to harm us.
Those of us who don’t buy that have an obvious basis of concern. A person unknown to us by the name of Emma Harrington had a similar concern and submitted, on 7 June 2021, a freedom of information request to Thames Water, that claims to be the UK’s largest water and waste water company.
The good news? The freedom of information request to Thames Water was successful. The bad news: Thames Water responded as follows: “Currently we have no monitoring programme.”
Reverse osmosis: size does matter
I find myself with one very clear recommendation if you have a concern, as I do. Consider, if you haven’t already, installing a high quality reverse osmosis (RO) system (see Figure 3) in your home and harvest your drinking and cooking water from that dedicated faucet.
Simply speaking an RO membrane is a semi-permeable membrane through which water is driven owing to pressure and a concentration gradient between the sediments and contaminants one side and pure water on the other. The membrane has tiny pores that are so small many mineral salts and contaminant molecules simply can’t travel through them to any significant extent, whereas as water molecules can.
This is one issue in which size does matter: the size of the pores in relation to your contaminant.
Here, let me delight in quoting the CDC, which states that RO has “a very high effectiveness in removing viruses”, bacteria, protozoa and “common chemical contaminants”.
What about the size of the SARS-CoV-2 viral particle, the spike protein, and the membrane pore size. Here are the summary stats:
- SARS-CoV-2 diameter: 100 nanometers (0.1 microns)
- SARS-CoV-2 spike protein length: 10 nanometers (0.01 microns)
- Typical pore size of RO membrane: 0.1 nanometers (0.0001 microns)
In short, that means a SARS-CoV-2 viral particle is around 1000 times larger than the pore size of an RO membrane. Possibly even more importantly, the SARS-CoV-2 spike protein is around 100 times the length of the RO pore diameter. This suggests that the vast majority of intact spike protein molecules will struggle to work their way through a RO membrane.
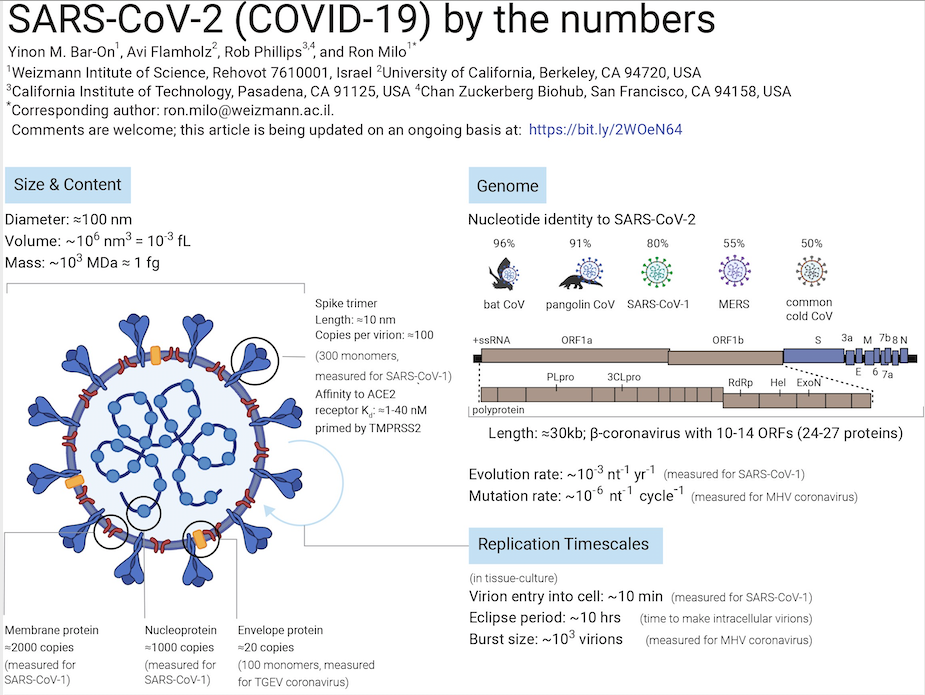
Figure 2. Various numbers linked to SARS-CoV-2 (from Bar-On et al. Science Forum: SARS-CoV-2 (COVID-19) by the numbers. eLife 2020; 9: e57309).
In practical terms, we strongly suggest, if you haven't already, you invest - if you can - in an under-sink RO system (e.g. Fig. 3), that also re-alkalises the water with health-giving mineral salts. Some commercially available systems also utilise various energetic systems (e.g. vortices, magnets) that help to re-structure the water, improving its utilisation in the body and its resultant health benefits.
All systems do require annual maintenance and sanitation to avoid any build up of bacteria, and typically in a domestic setting, the RO membrane will last around 3 years before needing replacement.

Figure 3a. Typical under-sink, multi-stage, domestic reverse osmosis drinking water nanofiltration system, including sediment filter, granular activated carbon filter, carbon block filter, RO membrane nanofilter, post-RO (polishing) filter and water tank.

Figure 3b. Typical under-sink, multi-stage, domestic reverse osmosis drinking water nanofiltration system, including sediment filter, granular activated carbon filter, carbon block filter, RO membrane nanofilter, post-RO (polishing) filter and water tank installed in the ANH office.

Figure 3c. An example of a direct flow, tankless RO and carbon block filter system that provides ambient temperature, hot and near-boiling water. Water flow rate is lower (~1 litre per minute) than tank-based systems. Source: Osmio Water Technology
Haldane epilogue
I kicked this piece off with a quote from JBS Haldane. It’s worth remembering that in his heyday in the mid-20th century, science was often seen as being entirely independent of politics. There was such a thing as ‘blue sky research’. Science back then had yet to be fully corrupted by political and economic powers. Yet Haldane’s extraordinary astuteness enabled him to forecast what has since become a dominant problem of our day. He asserted, “I began to realise that even if the professors leave politics alone, politics won’t leave the professors alone.”
Politics, inseparable from economics, is why the majority of scientists will continue to tell you remdesivir is the answer to your covid-19 infection and your drinking water supplies are safe without nanofiltration. Don’t think for a minute that’s got anything to do with science.
And if your survival instinct kicks in and your sense of reason tells you the mainstream rationale must be wrong, my sense is you stand a much better chance than most in this inverted, confusing and rapidly changing world.
Please share this article widely with those you care about. Thank you.
>>> Alliance for Natural Health International re-Publishing Guidelines
>>> Has this article generated questions for you? Did you know our ANH Pathfinder Members get a free monthly Q&A as part of their annual membership? Why not Join us!
>>> For more curated covid coverage from the past 2 years visit Covidzone.org
Proudly affiliated with: Enough Movement Coalition partner of: World Council for Health




Comments
your voice counts
14 April 2022 at 9:01 pm
I believe RO uses lots of water and so is eco-unfriendly as well as expensive for anyone on metered water. I was wondering if clever use of UVC light might be another option? Could this be a gadget that needs to be invented by someone or is it already available? If so, how does it compare? Many thanks.
14 May 2022 at 10:21 am
I have several different filters. A whole house system (from Pozzani) which filters to the shower and bath etc. These are about £50.
RO is just a filtration system. It doesn't use more water than it filters as far as I am aware. It just puts the water through two filters and then it has the RO section on top of that which removes more contaminants. Mine dispenses the water into a tank so it's always available. They are more expensive and require a lot more space under the sink. I also have a desktop style Berkey which keeps the minerals and takes out everything else. Again as far as I'm aware you can put river water into that and it removes bacteria/viruses etc. Pozzani also also do a UV filtration system, these are often used for fish tank water, so this tech is already available.
14 April 2022 at 10:05 pm
We have an Aqua-Pur line powered purifier which is table top and plugs into the mains. For emergencies we have a Berky gravity-fed purifier, both of which meet your recommended standards.
Why are we concerned with waste water, presumably it isn't recycled into the drinking water system!
15 April 2022 at 1:37 am
Great article, thank you. I was wondering if distillation would be as effective as RO for removing the spike proteins from my drinking water?
15 April 2022 at 8:43 am
Reverse osmosis is expensive. Rain water filtered through a doulton gravity filter container is a much more economical option. The tainting of water supply by traces of hormones from plastic and birth control chemicals from water extracted from rivers is also then not consumed. This is why fish are having sexual definition altered, the water companies when asked why this not removed they advised they could hardly measure it! Crocodiles in Florida producing sterile eggs. Is the seeming increase in deviation in human sexuality also partialy caused by this?
20 April 2022 at 11:02 am
I have heard that RO filtration takes all the minerals out of the water causing it to be positively harmful to human health. For this reason gravity fed filtration is better - although it may not take spike proteins out.
Like most things, it’s a compromise.
21 April 2022 at 11:29 am
Hi Willie
Thanks for your comment. RO systems can also remineralise the water once it's been filtered. Alternatively you can add an electrolyte solution to the water before you drink it.
Warm wishes
Melissa
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences