

Content Sections
Rob Verkerk PhD; founder, executive & scientific director, ANH-Intl
Every day we hear health authorities claiming that the current crop of novel platform covid vaccines are “safe and effective”. Last week we presented you with evidence that points to the increasing failure of the global mass vaccination program; at least in relation to its purported aim of stopping transmission and building herd immunity with a view to helping societies to exit the pandemic. In the light of this evidence, there is no scientific support for the “effective” claim which should be deemed scientific (or medical) misinformation.
This week, we look closer at the other side of the coin, the claim widely made by authorities that these novel vaccines are “safe”.
Safety signals ignored in the early clinical trials
You’ll recall that regulatory agencies around the world, following suit behind the US Food & Drug Administration, the UK’s Medicines and Healthcare Regulatory products Authority (MHRA) and the European Medicines Agency (EMA), issued ‘emergency use authorisations’ (EUAs) early on to BioNtech/Pfizer, Oxford/AstraZeneca, Moderna – and slightly later – to Janssen/Johnson&Johnson (J&J). These were, by definition, experimental products being used on the public in a claimed ‘emergency’ situation, one that the UK had already deemed was not the result of a ‘high consequence infectious disease.’
The data underpinning these decisions on both benefits and harms were very limited, derived from just two or three months’ worth of data. Efficacy data generally claiming in excess of 90% vaccine effectiveness was initially published in press releases by vaccine manufacturers. Subsequently, safety and efficacy data for all three ‘vaccines’ given EUAs in the USA were published in the prestigious New England Journal of Medicine; here for Pfizer, here for Moderna and here for J&J.
The stratospheric numbers reflecting efficacy – Pfizer and Moderna’s level pegging at 95% and J&J’s at 94.1%, like none that had ever been seen before for a vaccine – were enthusiastically delivered by the media to a public that had been conditioned to be fearful of the new coronavirus. In countries that had control of the supply of experimental products, carefully crafted advertising generated very high levels of uptake for these experimental gene therapy products that were widely perceived as the surest way out of the surreal existence so many had endured for close to a year.
However, as we showed last week, these figures would not be sustained for long in the real world, outside the clinical conditions of trials, especially not in the face of immune escape and functional mutations (new variants).
J Bart Classen MD, an immunologist and vaccine adverse events researcher who previously worked at the National Institutes of Health (NIH) and the National Institute for Allergy and infectious Diseases (NIAID), headed by Dr Anthony Fauci, has long been concerned about lack of transparency around vaccine data. He argued in the BMJ as early as 1999, that the public should be “fully informed that vaccines….may have long term adverse effects”, that “proper safety studies were needed” and greater transparency might result in the “development of safer vaccine technology.”
Dr Classen has recently turned his attention to the New England Journal of Medicine datasets of Pfizer, Moderna and J&J covid ‘vaccines’, supported by some additional data issued by relevant FDA advisory committees.
I don’t bemoan Dr Classen’s choice of journal to publish his results. The vast majority of high impact factor journals have done a great disservice to science by refusing to carry articles that are in any way critical of the novel ‘vaccines’. Classen’s analysis, accepted for publication in late August 2021, can be found in the recently launched Trends in Internal Medicine, a minor journal that has yet to be listed in the US National Library of Medicine catalog.
Classen – doing what he was trained to do while in service to Fauci’s department – did what any halfway decent researcher would initially do at the start of an investigation: compare severe adverse events in those who were injected with the ‘real thing’ from each of the 3 manufacturers as against those injected with saline placebos. No further digging was required to spot a problem. The top line findings are summarised in Table 1 below.
Table 1. Summary data on total numbers of severe events in clinical trial data for 3 covid-19 vaccines (data source: Classen 2021).
|
Manufacturer |
No. vaccinated |
No. of severe events |
Difference |
% excess in treatment group |
P value |
||
|
Treatment |
Control |
Treatment |
Control |
||||
|
Pfizer |
21,720 |
21,728 |
262 |
172 |
90 |
152% |
P = 0.000014 |
|
Moderna |
15,210 |
15,210 |
3,985 |
943 |
3,042 |
423% |
P = 0.00001 |
|
J&J |
19,630 |
19,691 |
595 |
331 |
264 |
180% |
P = 0.00001 |
The results show highly significant differences in reported severe events between treatment-injected and control- (placebo) injected groups. Severe events were categorised as either Grade 3 or Grade 4 events according to guidance by the FDA, where Grade 3 are described as sufficiently severe as to prevent daily activity and that require medical intervention, with Grade 4 described as potentially life threatening, requiring an emergency room visit or hospitalisation. The difference was most pronounced, though no more statistically significant, for the Moderna jabs, with over four times (423%) more people being affected by severe events in the treatment rather than the placebo group.
In short: data from all three ‘vaccines’ should have sounded a sky high safety signal, one concealed in the pages of none other than the New England Journal of Medicine. These data that were in the possession of all regulators who dispensed EUAs should, at the very least, have caused regulators from forcing the vaccine makers from calling their vaccines "safe". Health authorities, the medical profession, the media or any other party promoting the unqualified safety of the vaccines should have received the same message which is otherwise misleading, a distortion of science, and in many instances technically illegal. Instead, because the authors of all three papers discounted the seriousness of the adverse events in their conclusions, the signals were roundly ignored by health authorities, the media and the majority of the scientific and medical community.
Digging into the AER databases
So where do we go to keep track of the unfolding picture of adverse events? The primary portals for such data are the official, government-controlled adverse event reporting systems, of which there are many (Table 2). All data can be entered by the public or by health professionals, but not all of it is accessible to the public. It is well recognised, including by the US Vaccine Adverse Event Reporting System (VAERS) that under-reporting is the norm for all such passive reporting systems. Reporting for serious adverse events is likely to be higher than for less serious ones that might be as low as 1%. Health authorities also have the ability to scrub results after they’re reported if they don’t agree that the event is related to the vaccine exposure.
Table 2. Adverse event reporting (AER) systems in selected countries, including accessibility of data
|
AER system |
Country/ |
AER data can be |
Publicly accessible data |
Detailed AER data accessible e.g. age, gender, dosing, etc |
|
VAERS |
✓ |
✓ |
✓ |
|
|
Yellow Card |
✓ |
✓ |
✘ |
|
|
VigiAccess |
✓ |
✓ |
✘ |
|
|
EUDRA |
✓ |
✓ |
|
|
|
Database of Adverse Event Notifications (DAEN) |
✓ |
✓ |
✘ |
|
|
Canadian Adverse Events Following Immunization Surveillance System (CAEFISS) |
✓ |
✓ |
✓ (age only) |
|
|
Cutaneous adverse drug reaction (ADR) classicification |
✓ |
✘ |
✘ |
|
|
Signaler les effets indésirables d'un médicament |
✓ |
✘ |
✘ |
|
|
AEMPS |
✓ |
✓ |
✓ (age only) |
|
|
AIFA |
✓ |
✓ |
✓ (age only) |
|
|
Swedish Medical Products Agency |
✓ |
✓ |
✓ (age only) |
|
|
Ministry of Health |
✘ |
✘ |
✘ |
|
|
Statens legemiddelverk |
✓ |
✓ |
✓ (age & gender) |
|
|
AEFI |
✓ |
✘ |
✘ |
There has yet to be a vaccine that has targeted the entire adult population of the USA so we should expect something of an uptick in voluntary reports made to the US Vaccine Adverse Event Reporting System (VAERS) post introduction of novel covid ‘vaccines’. Figure 1 shows reported death by vaccines from 1990 to the present, revealing the nature of the uptick. It’s big, if not sensational.
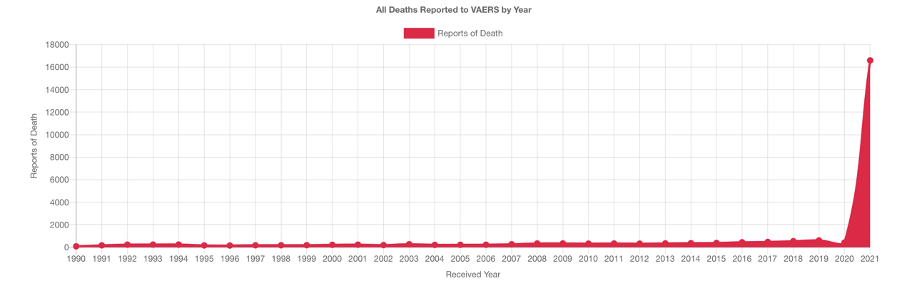
Figure 1. All deaths reported to VAERS by year (1990-2021). Source: OpenVAERS.
The VAERS database, that includes data that have been reported but not necessarily verified as being caused by the vaccine in question, include up to 1 October 2021; 778,683 reports in total, including 16,310 deaths, 75,605 hospitalisations and 87,814 urgent care visits.
Putting the current death figure into some, albeit dark, perspective, the number of people reportedly deceased as a result of covid ‘vaccines’ in the USA amounts to five and a half times more than those who died on September 11, 2011 in the World Trade Centre collapse in New York, 259 times the number who died on Pan Am flight 101 as a result of the Lockerbie bombing (in 1988), and some 2,330 times more than those who died in the Space Challenger disaster of 1986.
It also equates to around 4 times more deaths per 100,000 population (including both vaccinated and unvaccinated) than those killed on US roads. Yet governments, the mainstream medical establishment, and the media remain mute on such risks, still characterising these vaccines as ‘safe’.
Myocarditis and pericarditis reports in VAERS are now approaching 9,000. These and other deaths through to 1 October 2021 are revealed by the OpenVAERS summaries (Fig. 2). If you look at the risk in terms of a denominator that includes all vaccinated persons, nearly 402 million doses delivered, the risk can look small (about 2 cases for each 10,000 doses of vaccines administered).
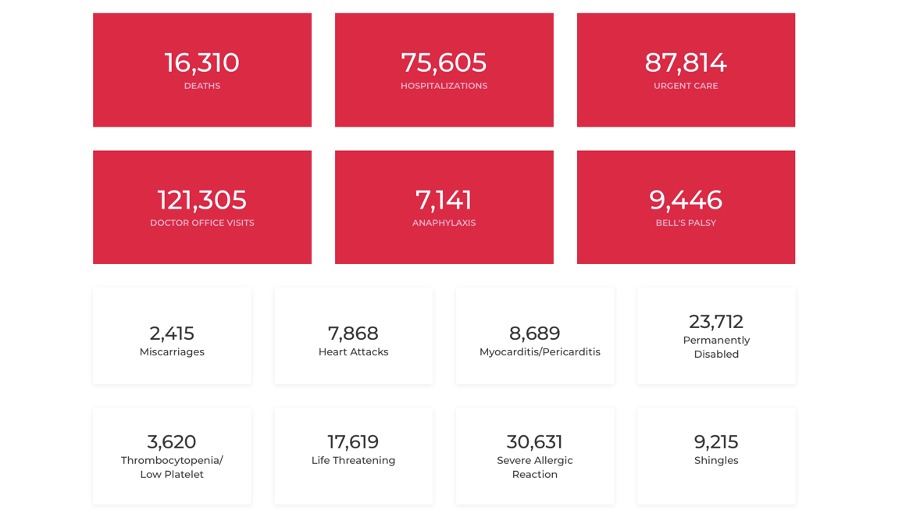
Figure 2. VAERS summaries based on 778,683 reports through to 1 October, 2021. Source: OpenVAERS.
But that's not how the risk pattern stacks up. As shown below (Fig. 3A), the risk of such events is disproportionately much greater for younger people and is greatest in the age group 10-15 years. As Drs Peter McCullough and Jessica Rose state in their paper just published in the journal Current Problems in Cardiology, "Within 8 weeks of the public offering of COVID-19 products to the 12-15-year-old age group, we found 19 times the expected number of myocarditis cases in the vaccination volunteers over background myocarditis rates for this age group."
The VAERS reports show the 12-32 year age group as the biggest affected age group, with an even larger slice of unknown age (that we presume were also young) (Fig 3D), these youngest groups deriving very little or no benefit from injections. Yet they face an appreciable risk (see Fig. 3A), especially from the second dose assuming this is administered (Fig. 3B), a risk that is entirely new for 2021 (Fig. 3C), especially from the Pfizer jab (Fig. 3B).
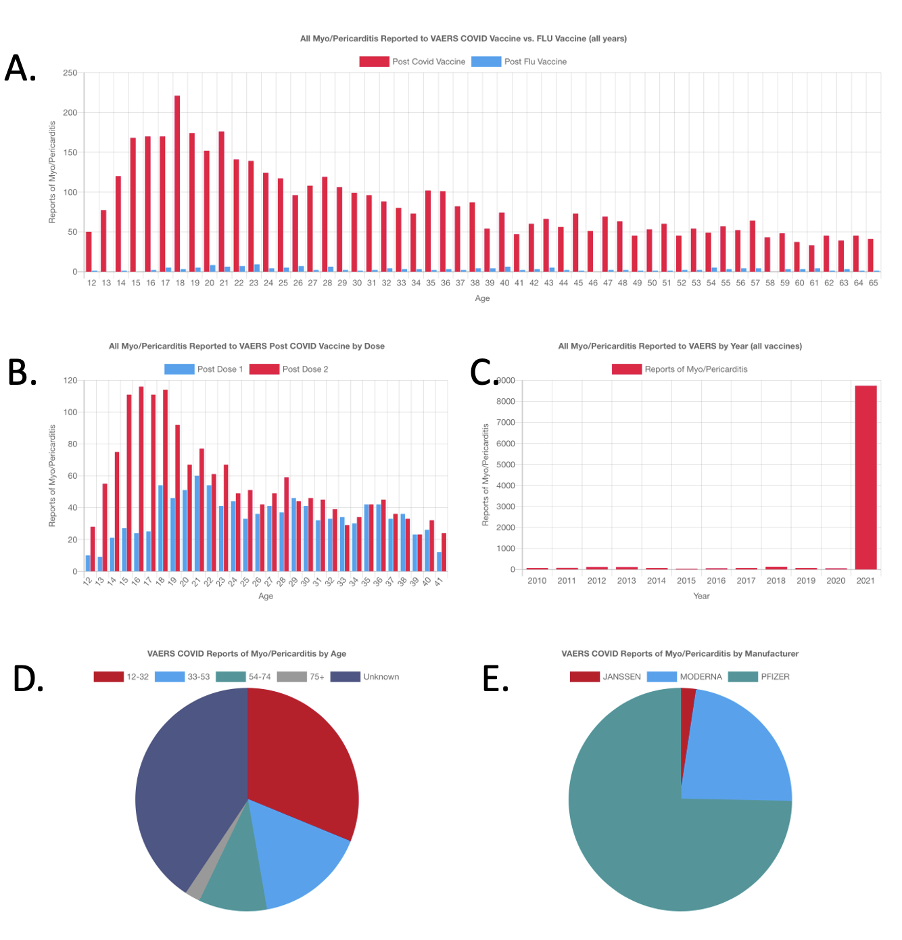
Figure 3. Myo-/peri-carditis reports through to 1 October 2021. A: Post covid and post-flu jab myo/pericarditis reports. B: Reports after first and second doses. C: Reports by year. D = Reports by age. E: reports by ‘vaccine’. Source: OpenVAERS.
A breakdown of AERs by age groups is shown in Table 3. While the numbers appear to be distributed fairly evenly across different age groups, as so many fewer younger people have been vaccinated, the adverse events are disproportionately higher for younger groups.
Table 3. Breakdown of deaths reported in VAERS up to 1 October 2021 (collation by ANH-Intl; source data: VAERS)
|
Sum of Events Reported |
Event Category |
||||||
|
Age |
Death |
Emergency Room * |
Emergency Room / Office Visit ** |
Hospitalized |
Life Threatening |
Permanent Disability |
Grand Total |
|
< 6 months |
2 |
14 |
0 |
13 |
3 |
3 |
35 |
|
6-11 months |
0 |
1 |
0 |
4 |
0 |
2 |
7 |
|
1-2 years |
2 |
10 |
0 |
4 |
1 |
3 |
20 |
|
3-5 years |
0 |
3 |
0 |
4 |
0 |
5 |
12 |
|
6-17 years |
32 |
2,821 |
2 |
1,485 |
285 |
133 |
4,758 |
|
18-29 years |
164 |
10,980 |
7 |
4,726 |
1,076 |
1,625 |
18,578 |
|
30-39 years |
267 |
14,105 |
12 |
5,378 |
1,595 |
2,515 |
23,872 |
|
40-49 years |
400 |
14,174 |
9 |
6,040 |
1,946 |
2,819 |
25,388 |
|
50-59 years |
852 |
13,307 |
12 |
7,392 |
2,249 |
2,870 |
26,682 |
|
60-64 years |
719 |
5,824 |
5 |
4,077 |
1,142 |
1,233 |
13,000 |
|
65-79 years |
3,495 |
13,233 |
5 |
13,536 |
2,979 |
2,674 |
35,922 |
|
80+ years |
4,251 |
4,967 |
3 |
8,246 |
1,364 |
973 |
19,804 |
|
Unknown |
6,126 |
8,319 |
2 |
24,700 |
4,978 |
8,857 |
52,982 |
|
Grand Total |
16,310 |
87,758 |
57 |
75,605 |
17,618 |
23,712 |
221,060 |
|
Proportion per vaccine dose |
4.05904E-05 |
0.00022 |
0.00000014 |
0.00018816 |
0.00004385 |
0.00006 |
0.00055 |
|
% per vaccine dose |
0.004059039 |
0.02184 |
0.00001419 |
0.01881567 |
0.00438456 |
0.00590 |
0.05501 |
|
AERs per 100k partially or fully vaccinated population* |
7.5 |
40.2 |
0.03 |
34.7 |
8.1 |
10.9 |
101.4 |
* Numbers partially or full vaccinated - source: Centers for Disease Control
UK data reported via the Yellow Card system shows the Moderna ‘vaccine’ to have yielded the highest adverse event report compared with the other two - two for every 100 doses administered. Total reported deaths are currently sitting at 1,663 which equates to around 2.5 per 100,000 population (both vaccinated and unvaccinated) which is on par with the number killed in the UK in road fatalities. Unlike cars that are widely regarded as inherently dangerous, these novel ‘vaccines’ continue to be regarded as ‘safe’.
Table 4. AER summary data from the UK MHRA Yellow Card system.
|
Manufacturer |
Total no. of vaccine doses |
No. of AERs |
AER rate % |
No. of Yellow Card reports received |
Total deaths |
|
Pfizer/BioNTech |
42,100,000 |
335,344 |
0.8 |
118,970 |
552 |
|
Moderna |
2,600,000 |
53,032 |
2.0 |
16,582 |
19 |
|
AstraZeneca |
48,900,000 |
830,818 |
1.7 |
233,904 |
1,097 |
|
Source data: MHRA as of 12 October 2021 (https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions) |
|||||
There is much more that could be said, but in the name of keeping this word count manageable, we propose you look elsewhere for more detail. The Swiss Policy Research report of covid vaccine adverse events describes an array of other reactions that have been reported, including untimely menstrual bleeding, miscarriages, birth defects, blood clots, strokes, heart attacks, severe skin reactions, Bell’s palsy, eye disorders, and more.
“Unavoidably unsafe”?
Having skimmed the surface of the reported data, it is clear that this new clutch of covid vaccines are at least as risky as driving around in motor vehicles. If we assume 10% or 1% of cases are under reported, they will then be 10 times or 100 times more dangerous than driving a car.
It would seem, then, that vaccines, especially the new-generation mRNA-based ones, are unavoidably unsafe, despite this not being recognised by health authorities or even the courts. There is a commonly held view, especially among vaccine-concerned non-lawyers in the USA, that the Supreme Court ruled that vaccines were “unavoidably unsafe” in the Bruesewitz v Wyeth case (2010). However, according to Rick Jaffe Esq, this is a misinterpretation of the ruling.
How much risk do we accept?
Prof David Spiegelhalter and his team from the Winton Centre for Risk and Evidence Communication, an internationally recognised authority on risk communication, shows just how clearly the risk of covid is minimal for the young and increases with age.
Spiegelhalter and colleagues were asked by the UK government in April this year to help communicate the blood clot risk linked to the Astra Zeneca jabs to the public. What his team came up with back then is summarised on this page, with one of the key figures shown below (Fig. 4)
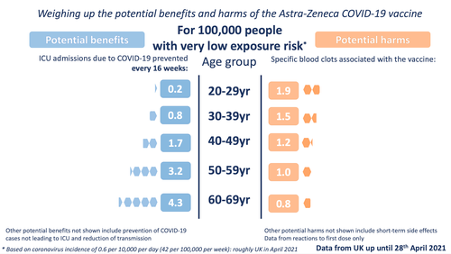
Figure 4. Potential benefits and harms from AstraZeneca jabs for different age groups (based on MHRA Yellow Card reports to 28 April 2021). Source: Winton Centre
This has to be a dramatic understatement of the current situation, but even back in April, harms outweighed benefits for anyone aged under 49 as you can see from Prof Spiegelhalter’s graphic (Fig. 4).
In early September, even the UK government’s own advisory group on vaccines, the Joint Committee on Vaccination and Immunisation (JCVI) determined there was insufficient evidence to justify the covid injection of 12- to 15-year-olds.
Despite the available science, the mass vaccination program rolls on relentlessly, seemingly to fulfil the goal, expressed many months earlier by Bill Gates and others, to vaccinate almost everyone on the planet. In the UK, as in so many countries, young people continue to be pushed hard and coerced into receiving covid ‘vaccines’ or face discrimination, penalties or restrictions. This is no longer a matter of science.
Mass misinformation
Those of us who have been critical of government and health authority communications around covid ‘vaccine’ safety have been widely targeted as misinformation sources. Many of our social media channels have been de-platformed for making claims that are supported by robust science – us included in the case of YouTube. But as always, especially given the complexity and uncertainty of the science, the situation is so much more nuanced than it might appear if you’ve only been listening or reading mainstream media.
I’ll leave you with four overriding concerns we have that are rooted in misinformation from those responsible for the primary narrative:
- That the novel covid ‘vaccines’ are both “safe and effective”
- That young people (under the age of 50) should receive covid ‘vaccines’ on the basis of the balance between potential benefits and harms, or otherwise face penalties or restrictions of their freedoms
- That people who’ve already been exposed to SARS-CoV-2 and have achieved natural immunity should be much better protected if vaccinated – when the benefits of vaccination post naturally-acquired infection remain unclear
- That the vast majority of public health authorities, medical doctors, pharmacists and registered nurses who are recommending or administering covid ‘vaccines’ are doing so without adequate knowledge of their risks and benefits to particular sub-populations making then unable to provide the information necessary for vaccinees to exercise their right to medical informed consent.
Israel provides us with an early signal of what may happen elsewhere, in a best case scenario, because it was the first country to be intensively inoculated with the experimental jabs. It is then very relevant to discover just how fast cases are rising, leading to hospitalisations and further (nosocomial) transmission, especially among those who are fully vaccinated.
Only a few countries are being cautious with respect to safety concerns. Finland, Iceland, Sweden, Denmark and Norway have all suspended the use of the Moderna covid vaccine due to concerns over the incidence of myocarditis and pericarditis in young men.
We must work together to re-instate the right to medical informed consent, ensuring that those to whom these novel ‘vaccines’ are being offered, have access to all the relevant information on both safety and benefit that is available at a given time. We are a million miles from that point at present.
We are working with our affiliates at the World Council for Health and the UK Medical Freedom Alliance to raise awareness on these important issues.
>>> Access here UK template letters for parents and for children (Word documents) to decline Covid-19 vaccination in UK schools - that can be adapted for other countries, produced by our colleagues at the UK Medical Freedom Alliance.
Epilogue
Finally, here are two videos that we felt might be of interest. The first is by Project Veritas and concerns a whistleblower who has covertly filmed what appears to be a typical day in a hospital department.
The second concerns questions around ‘vaccine’- versus naturally-acquired immunity posed by Senator Rand Paul, a Kentucky Republican, to Health & Human Services Secretary Xavier Becerra during a Senate Health, Education, Labor, and Pensions Committee on 1 October (2021).
We appreciate any support you can give us – please consider joining us as a member for nominal annual or monthly fee – and please share this article widely.
For more curated content on the coronavirus crisis visit covidzone.org
Become a Pathfinder member
Return to Hompage
#enoughmovement #solidarity



Comments
your voice counts
15 October 2021 at 3:01 am
I'd be interested in some advice. A while back I was reporting Dr. Jessica Rose's analysis of the temporal association between adverse reactions and the date of vaccination. The link is at https://jameslyonsweiler.com/2021/05/17/study-finds-patterns-in-vaers-data-that-provide-evidence-of-causality, and the important graph is the black one with the yellow and orange lines. My concern with this is that the orange spike in deaths could be the result of a reporting bias, i.e. in the case of a death a couple of days after the vaccine, the proximity to the vaccine is often front-of-mind. 50 days later many people would be struggling to make a connection between the two, despite such a connection being possible. If it were possible to discount the reporting bias somehow, then this graph would be persuasive evidence.
15 October 2021 at 6:07 pm
Hi Martin - you are right, there can be reporting bias, just as there can be underreporting bias the more delayed the manifestation of an adverse event - especially complex ones that might result, for example, from triggering an autoimmune disease. One of the ways of checking against such biases is to determine the expected/background incidence of particular events, conditions and causes of death. This has already been unpacked very clearly for myocarditis/pericarditis (and there is a very clear vaccine AE signal) - but hasn't yet been done definitively (as far as I am aware) for overall causes of mortality for different population groups (accounting for age, gender, demographics, etc). Another important trend that we've seen is excess mortalities evident in the euroMOMO datasets (29 countries - mainly EU but also including Israel and Ukraine) for 2021. This didn't happen in 2020 when the first and second waves hit many countries and before vaccines were rolled out. The excess of deaths are likely to be multifactorial and could be related to such factors as: ADE, immune suppression, spike protein toxicity, autoimmunity, sustained chronic stress - and AERs (including many that will unreported to official AER systems).
15 October 2021 at 12:52 pm
Thank you Doctor. A very insightful article that brought forward evidence based conclusions. I appreciate the time you have gone to in putting this together.
16 October 2021 at 2:19 pm
Good article, but I believe the article needed more context.
Starting with a brief summary about vaccine effectiveness, so people can consider how the adverse side effects compare with any known benefits of vaccines.
For example, in the US, more people have already died from COVID in the first nine months of 2021, than in all of 2020, in spite of the vaccines. That makes no sense if the claim that vaccines are effective is true.
With the questionable effectiveness in mind, the number of side effects has a different meaning.
But to realize that meaning, the much lower side effects from vaccines in prior years should be presented as a comparison -- some details -- not just a simple chart.
Such as details on deaths, disabilities and hospitalizations reported for all vaccines in 2020, 2019, and perhaps for the worst year in the past 30 years. That detail would show exactly how unprecedented 2021 is, and the year is not over yet.
Unfortunately, a long discussion on how to use VAERS data is always required. Such as some details on studies estimating what percentage of side effects are reported. I'd say between 1% and 10% but there are other estimates
Then, if you study the actual VAERS submissions, it's obvious that more than half should be described as minor, such as a sore or numb arm for a short period of time. So the total side effects reported number includes many minor issues.
I believe the concentration should be on deaths, permanent disabilities and hospitalizations. And I am especially concerned about those problems happening to younger people (under 40) soon after the vaccinations, who were previously healthy.
Even with all the information, and estimates on the percentage of side effects that don't get reported, we still can't answer the important question:
Will vaccinated people, age adjusted, have a healthier life as a result of getting vaccinated (which I assume will include repeated booster shots)?
Until we determine adverse long term side effects, which can take years, and easily be missed, I don't see how to answer that question.
I had problems reading some of your charts.
I have a brief easy to read summary of the latest VAERS data on
one of my blogs:
https://electioncircus.blogspot.com/2021/10/vaers-covid-vaccine-adverse-side_15.html
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences